

Therapeutic targeting of inflammation in hypertension: from novel mechanisms to translational perspective
- PMID: 34698811
- PMCID: PMC9825256
- DOI: 10.1093/cvr/cvab330
Therapeutic targeting of inflammation in hypertension: from novel mechanisms to translational perspective
Abstract
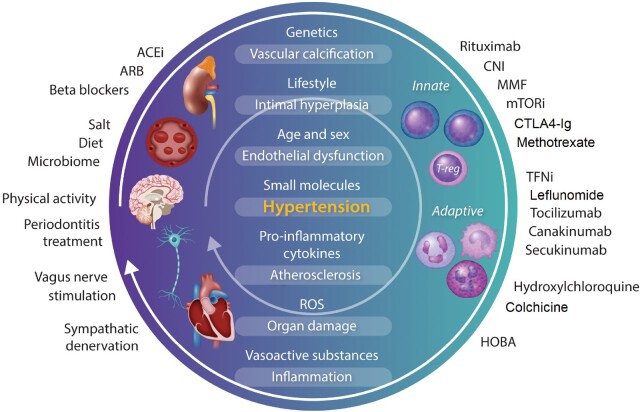
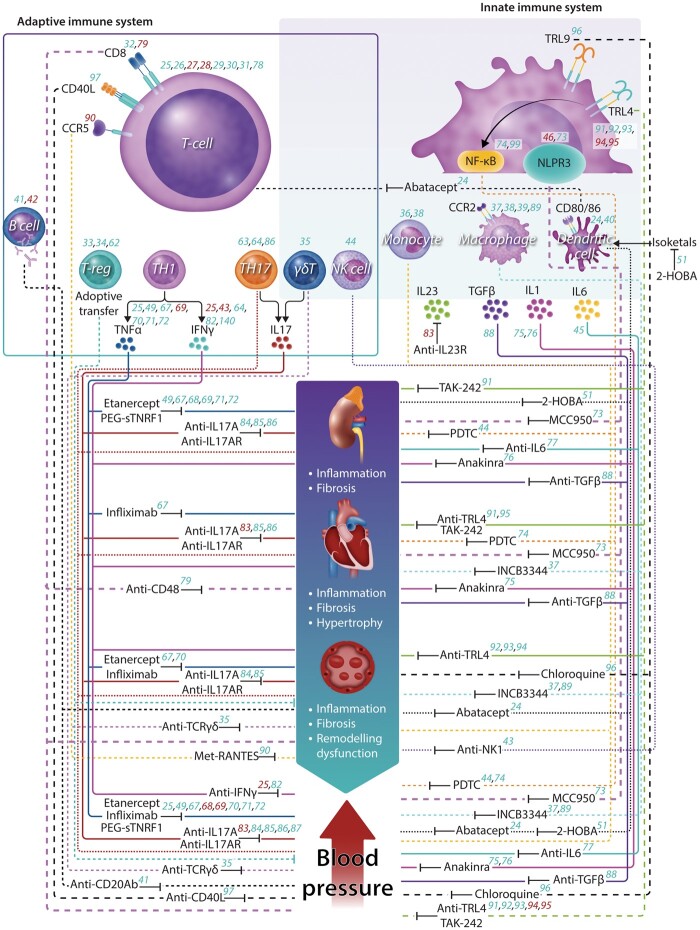
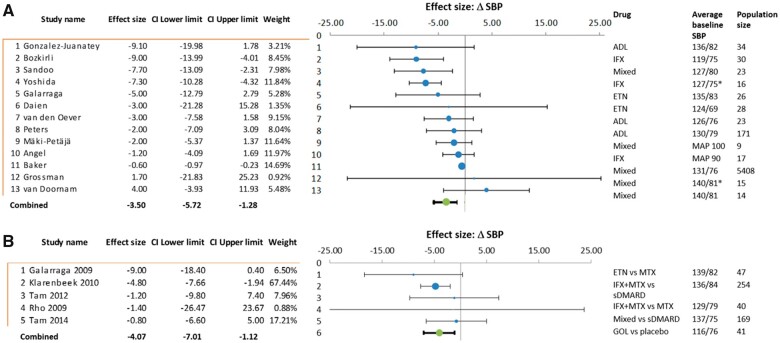
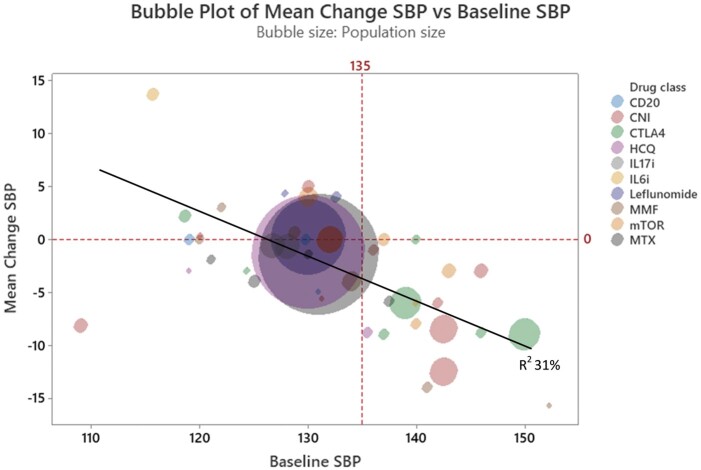
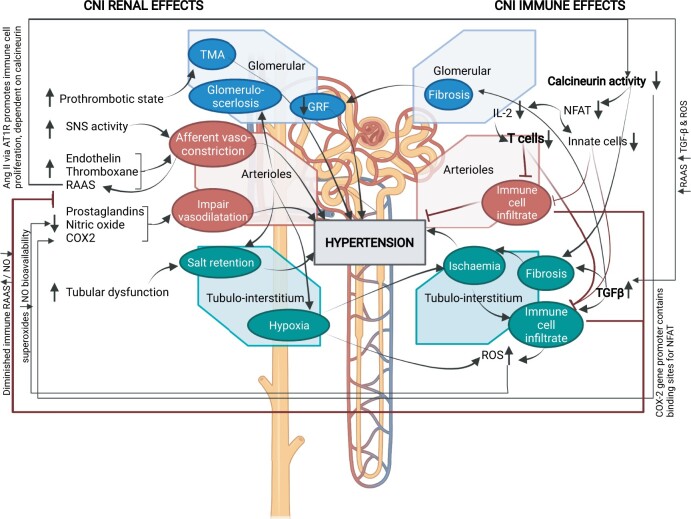
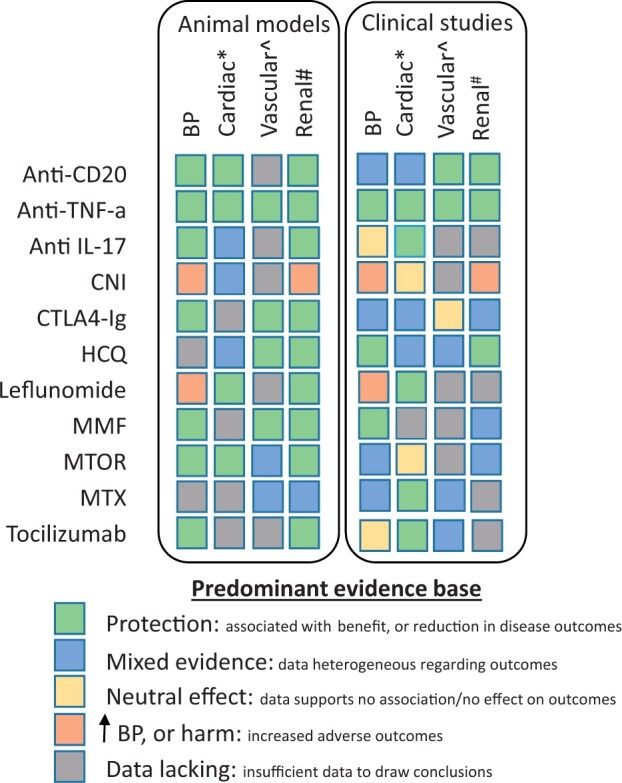
Both animal models and human observational and genetic studies have shown that immune and inflammatory mechanisms play a key role in hypertension and its complications. We review the effects of immunomodulatory interventions on blood pressure, target organ damage, and cardiovascular risk in humans. In experimental and small clinical studies, both non-specific immunomodulatory approaches, such as mycophenolate mofetil and methotrexate, and medications targeting T and B lymphocytes, such as tacrolimus, cyclosporine, everolimus, and rituximab, lower blood pressure and reduce organ damage. Mechanistically targeted immune interventions include isolevuglandin scavengers to prevent neo-antigen formation, co-stimulation blockade (abatacept, belatacept), and anti-cytokine therapies (e.g. secukinumab, tocilizumab, canakinumab, TNF-α inhibitors). In many studies, trial designs have been complicated by a lack of blood pressure-related endpoints, inclusion of largely normotensive study populations, polypharmacy, and established comorbidities. Among a wide range of interventions reviewed, TNF-α inhibitors have provided the most robust evidence of blood pressure lowering. Treatment of periodontitis also appears to deliver non-pharmacological anti-hypertensive effects. Evidence of immunomodulatory drugs influencing hypertension-mediated organ damage are also discussed. The reviewed animal models, observational studies, and trial data in humans, support the therapeutic potential of immune-targeted therapies in blood pressure lowering and in hypertension-mediated organ damage. Targeted studies are now needed to address their effects on blood pressure in hypertensive individuals.
Keywords: Blood pressure; Hypertension; Immune system; Immunomodulatory; Inflammation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Libby P. The changing landscape of atherosclerosis. Nature 2021;592:524–533. - PubMed
-
- Nus M, Mallat Z, Sage A. Beating (T-lymphocyte driven) atherosclerosis with B- and T-lymphocyte attenuator. Cardiovasc Res 2020;116:251–252. - PubMed
-
- Douna H, Amersfoort J, Schaftenaar FH, Kröner MJ, Kiss MG, Slütter B, Depuydt MAC, Bernabé Kleijn MNA, Wezel A, Smeets HJ, Yagita H, Binder CJ, Bot I, van Puijvelde GHM, Kuiper J, Foks AC. B- and T-lymphocyte attenuator stimulation protects against atherosclerosis by regulating follicular B cells. Cardiovasc Res 2020;116:295–305. - PubMed
