

Impact of Hydrocortisone and of CRH Infusion on the Hypothalamus-Pituitary-Adrenocortical Axis of Septic Male Mice
- PMID: 34698826
- PMCID: PMC8599906
- DOI: 10.1210/endocr/bqab222
Impact of Hydrocortisone and of CRH Infusion on the Hypothalamus-Pituitary-Adrenocortical Axis of Septic Male Mice
Abstract
Purpose: Sepsis is hallmarked by high plasma cortisol/corticosterone (CORT), low adrenocorticotropic hormone (ACTH), and high pro-opiomelanocortin (POMC). While corticotropin-releasing hormone-(CRH) and arginine-vasopressin (AVP)-driven pituitary POMC expression remains active, POMC processing into ACTH becomes impaired. Low ACTH is accompanied by loss of adrenocortical structure, although steroidogenic enzymes remain expressed. We hypothesized that treatment of sepsis with hydrocortisone (HC) aggravates this phenotype whereas CRH infusion safeguards ACTH-driven adrenocortical structure.
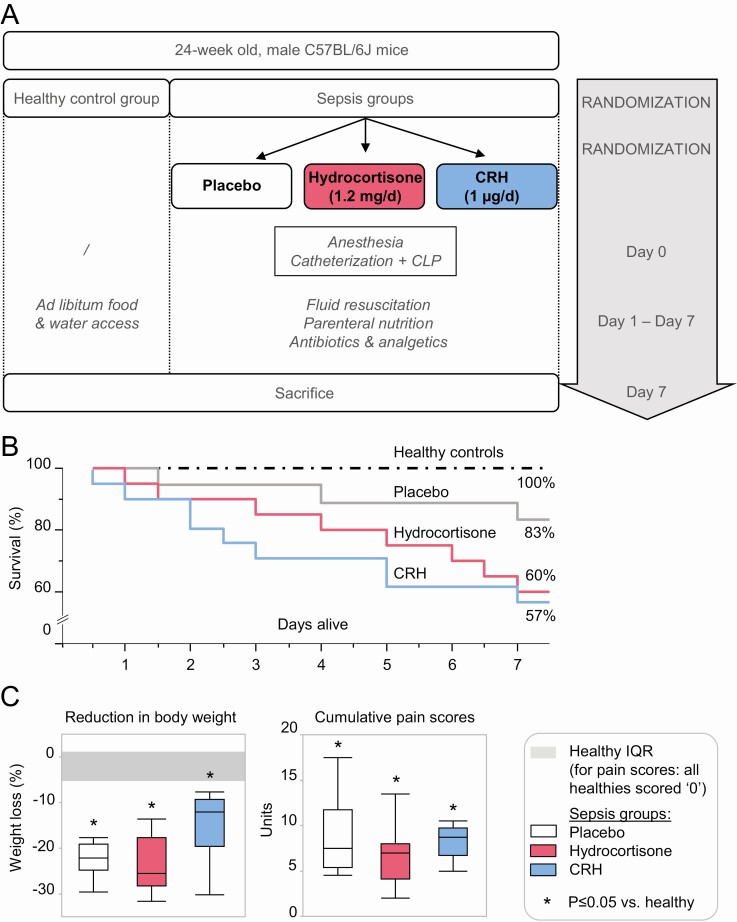
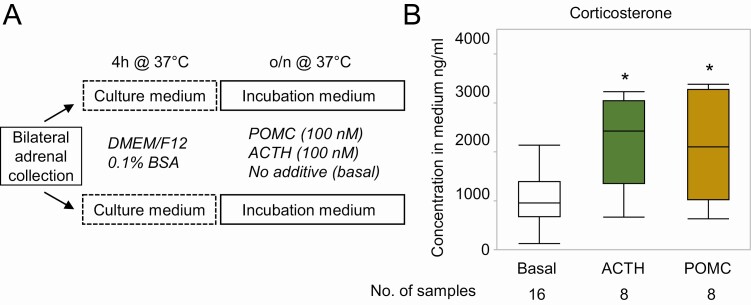
Methods: In a fluid-resuscitated, antibiotics-treated mouse model of prolonged sepsis, we compared the effects of HC and CRH infusion with placebo on plasma ACTH, POMC, and CORT; on markers of hypothalamic CRH and AVP signaling and pituitary POMC processing; and on the adrenocortical structure and markers of steroidogenesis. In adrenal explants, we studied the steroidogenic capacity of POMC.
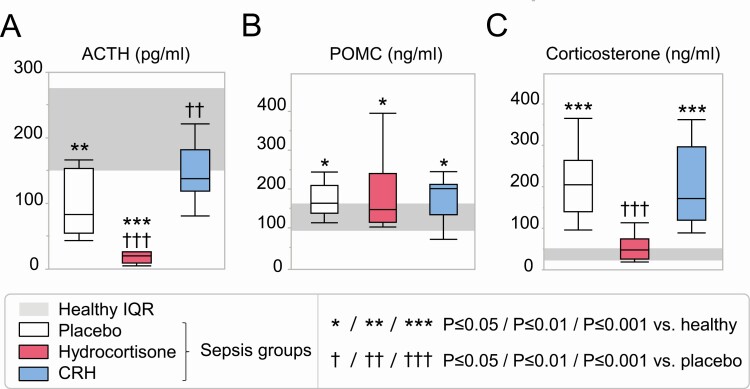
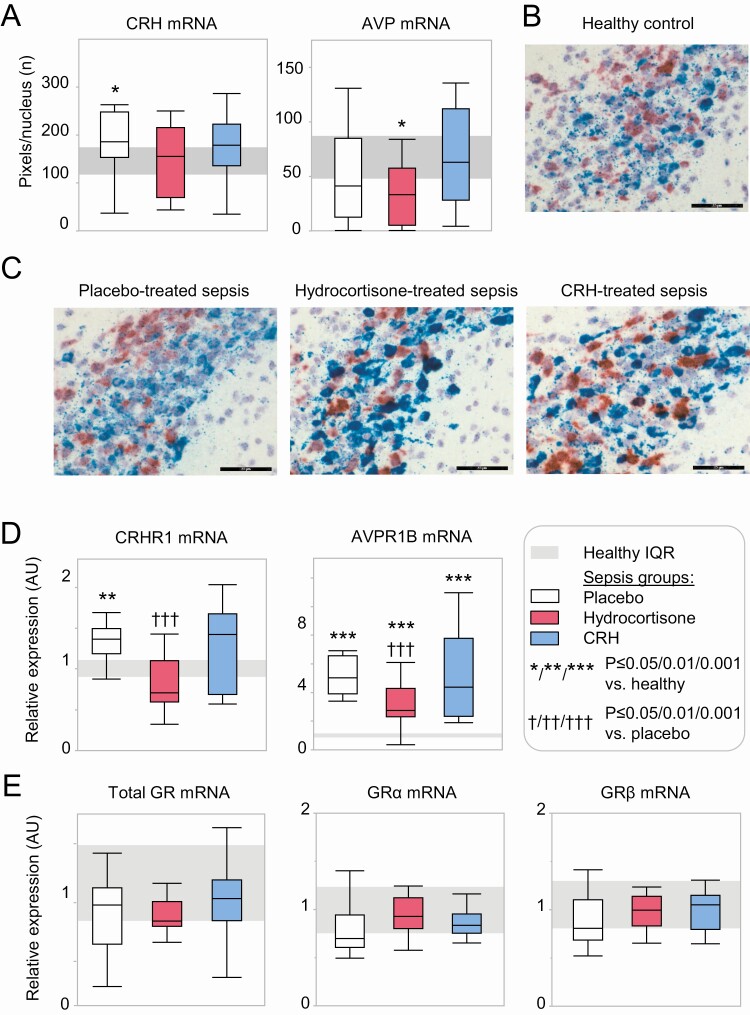
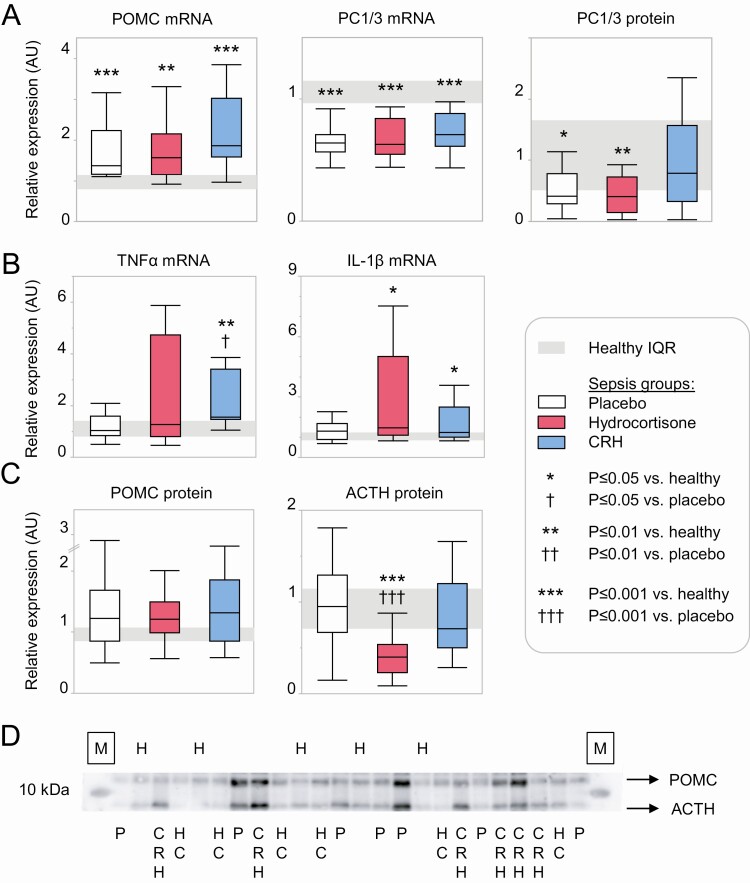
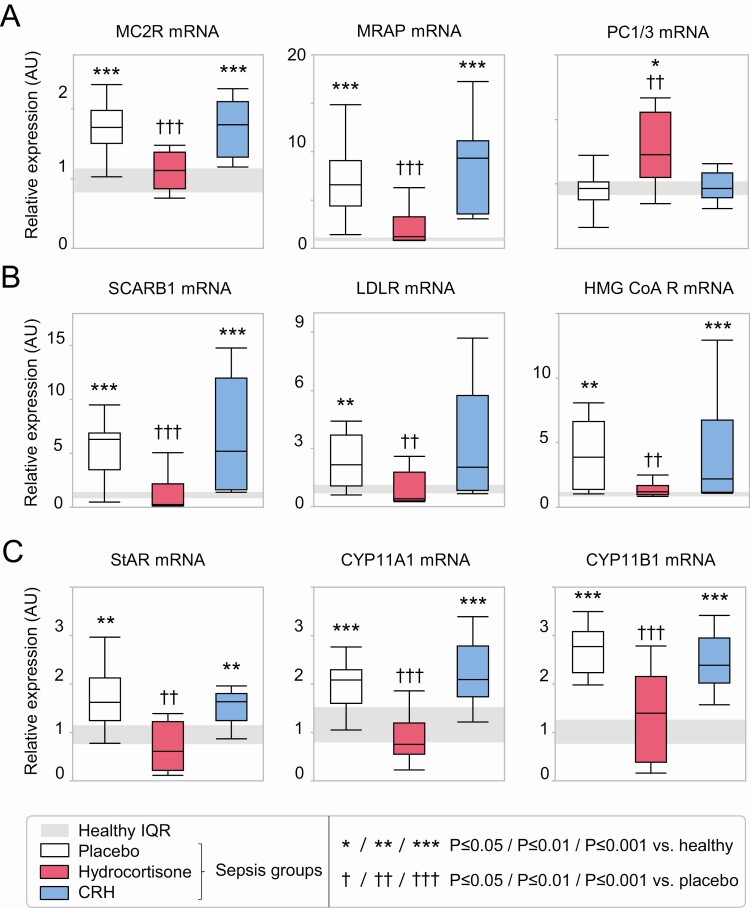
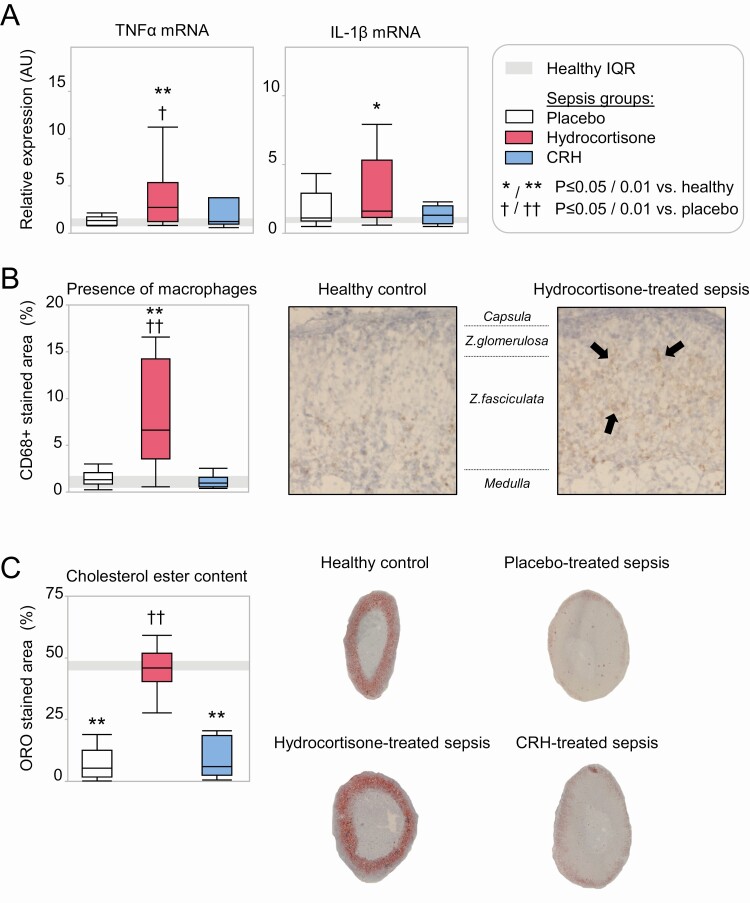
Results: During sepsis, HC further suppressed plasma ACTH, but not POMC, predominantly by suppressing sepsis-activated CRH/AVP-signaling pathways. In contrast, in CRH-treated sepsis, plasma ACTH was normalized following restoration of pituitary POMC processing. The sepsis-induced rise in markers of adrenocortical steroidogenesis was unaltered by CRH and suppressed partially by HC, which also increased adrenal markers of inflammation. Ex vivo stimulation of adrenal explants with POMC increased CORT as effectively as an equimolar dose of ACTH.
Conclusions: Treatment of sepsis with HC impaired integrity and function of the hypothalamic-pituitary-adrenal axis at the level of the pituitary and the adrenal cortex while CRH restored pituitary POMC processing without affecting the adrenal cortex. Sepsis-induced high-circulating POMC may be responsible for ongoing adrenocortical steroidogenesis despite low ACTH.
Keywords: ACTH; CRH; HPA axis; POMC; hydrocortisone; sepsis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Septic Shock: A Disruptor of the Hypothalamic-Adrenal Axis as We Know It.Endocrinology. 2022 May 1;163(5):bqac010. doi: 10.1210/endocr/bqac010. Endocrinology. 2022. PMID: 35134141 Free PMC article. No abstract available.
References
-
- Fleischmann C, Scherag A, Adhikari NK, et al. ; International Forum of Acute Care Trialists . Assessment of global incidence and mortality of hospital-treated sepsis. current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259-272. - PubMed
-
- Téblick A, Peeters B, Langouche L, Van den Berghe G. Adrenal function and dysfunction in critically ill patients. Nat Rev Endocrinol. 2019;15(7):417-427. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
