

COVID-19 and the lungs: A review
- PMID: 34700289
- PMCID: PMC8486577
- DOI: 10.1016/j.jiph.2021.09.024
COVID-19 and the lungs: A review
Abstract
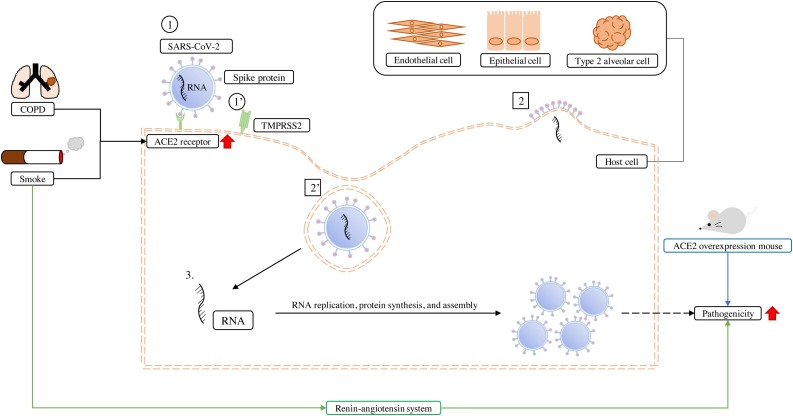
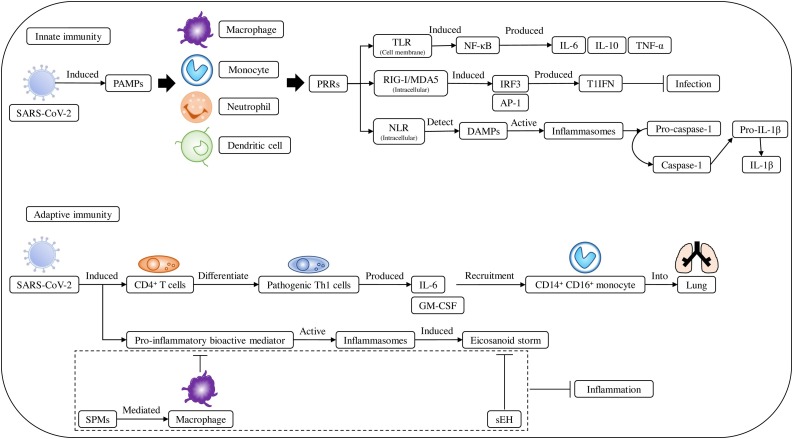
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) attacks pulmonary alveolar cells via angiotensin-converting enzyme 2 (ACE2) receptors and causes pulmonary infections that result in coronavirus disease (COVID-19), inducing immune responses that can result in severe pneumonia. We reviewed the clinical experiences of lung diseases during the COVID-19 pandemic to offer insights into the adaptations made by experts in the diagnosis and treatment of these comorbidities. Various lung comorbidities increase the severity of COVID-19 and associated mortality by amplifying ACE2 expression. Additionally, the COVID-19 pandemic has changed the use of routine diagnostic pulmonary imaging methods, making chest sonography scoring the most convenient, as it can be conducted bedside. Treatment protocols for SARS-CoV-2 infection and the underlying lung diseases are also affected owing to potential interactions. The optimal diagnostic methods and treatment protocols for lung diseases have been adapted worldwide to increase survival rates and attenuate acute lung injuries during the COVID-19 pandemic.
Keywords: Angiotensin-converting enzyme 2; Coronavirus disease-19; Lung comorbidities; Pathophysiology; Pulmonary images; Severe acute respiratory syndrome coronavirus-2.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Johns Hopkins University Coronavirus Resource Center . 2021. Mortality analyses.https://coronavirus.jhu.edu/data/mortality [accessed 26 January 2021]
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
