

FDA-approved bone grafts and bone graft substitute devices in bone regeneration
- PMID: 34702541
- PMCID: PMC8555702
- DOI: 10.1016/j.msec.2021.112466
FDA-approved bone grafts and bone graft substitute devices in bone regeneration
Abstract
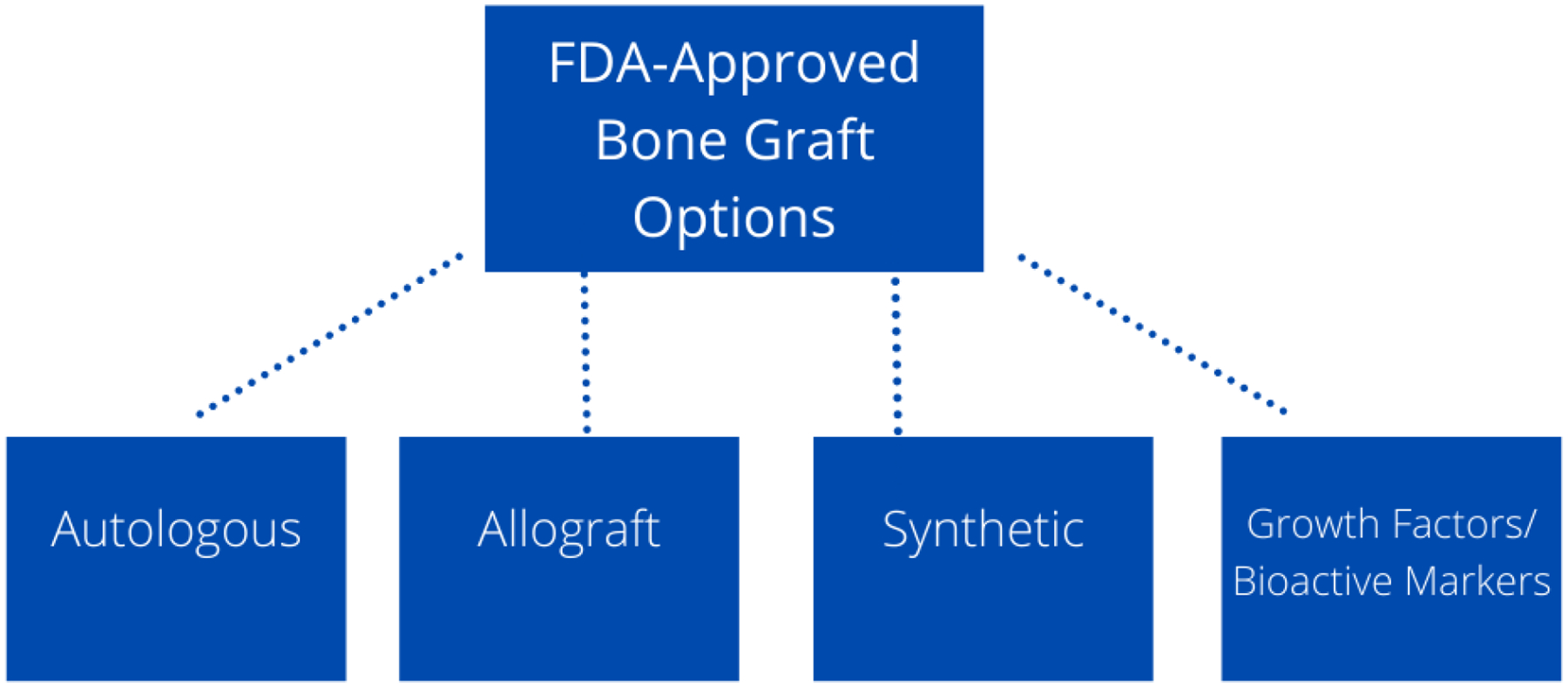
To induce bone regeneration there is a complex cascade of growth factors. Growth factors such as recombinant BMP-2, BMP-7, and PDGF are FDA-approved therapies in bone regeneration. Although, BMP shows promising results as being an alternative to autograft, it also has its own downfalls. BMP-2 has many adverse effects such as inflammatory complications such as massive soft-tissue swelling that can compromise a patient's airway, ectopic bone formation, and tumor formation. BMP-2 may also be advantageous for patients not willing to give up smoking as it shows bone regeneration success with smokers. BMP-7 is no longer an option for bone regeneration as it has withdrawn off the market. PDGF-BB grafts in studies have shown PDGF had similar fusion rates to autologous grafts and fewer adverse effects. There is also an FDA-approved bioactive molecule for bone regeneration, a peptide P-15. P-15 was found to be effective, safe, and have similar outcomes to autograft at 2 years post-op for cervical radiculopathy due to cervical degenerative disc disease. Growth factors and bioactive molecules show some promising results in bone regeneration, although more research is needed to avoid their adverse effects and learn about the long-term effects of these therapies. There is a need of a bone regeneration method of similar quality of an autograft that is osteoconductive, osteoinductive, and osteogenic. This review covers all FDA-approved bone regeneration therapies such as the "gold standard" autografts, allografts, synthetic bone grafts, and the newer growth factors/bioactive molecules. It also covers international bone grafts not yet approved in the United States and upcoming technologies in bone grafts.
Keywords: Bone cement; Bone grafts; Bone morphogenetic proteins; Clinical indications; Food and drug administration; Platelet derived growth factor.
Copyright © 2021 Elsevier B.V. All rights reserved.
Figures




References
-
- Greenwald AS, Boden SD, Goldberg VM, Khan Y, Laurencin CT, Rosier RN, and American I. Academy of Orthopaedic Surgeons. The Committee on Biological, Bone-graft substitutes: facts, fictions, and applications. J Bone Joint Surg Am, 2001. 83-A Suppl 2 Pt 2: p. 98–103. - PubMed
-
- Finkemeier CG, Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am, 2002. 84(3): p. 454–64. - PubMed
-
- Faour O, Dimitriou R, Cousins CA, and Giannoudis PV, The use of bone graft substitutes in large cancellous voids: any specific needs? Injury, 2011. 42 Suppl 2: p. S87–90. - PubMed
-
- Van Heest A and Swiontkowski M, Bone-graft substitutes. The Lancet, 1999. 353: p. S28–S29. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
