

Impact of HBsAg and HBcrAg levels on phenotype and function of HBV-specific T cells in patients with chronic hepatitis B virus infection
- PMID: 34702717
- PMCID: PMC9554084
- DOI: 10.1136/gutjnl-2021-324646
Impact of HBsAg and HBcrAg levels on phenotype and function of HBV-specific T cells in patients with chronic hepatitis B virus infection
Abstract
Objective: Hepatitis B virus (HBV)-specific T cells are main effector cells in the control of HBV infection and hepatitis B surface antigen (HBsAg) is suggested to be a critical factor in the impaired immune response, a hallmark of chronic HBV infection. In addition to HBsAg, other viral markers such as hepatitis B core-related antigen (HBcrAg) are available, but their potential association with HBV-specific immune responses is not defined yet, which will be important if these markers are used for patient stratification for novel therapies aimed at functional HBV cure.
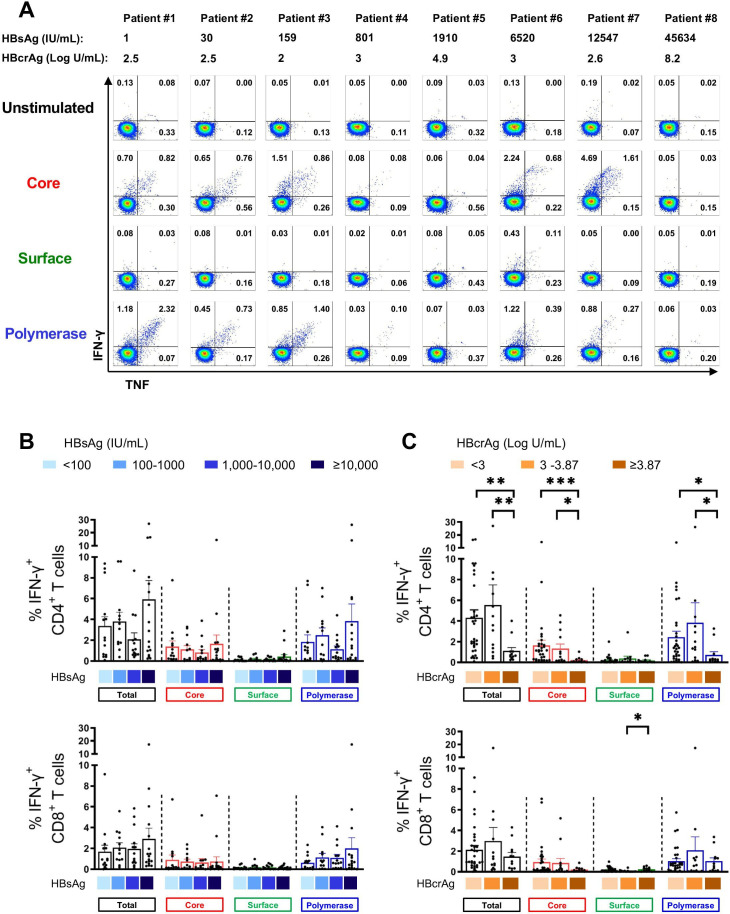
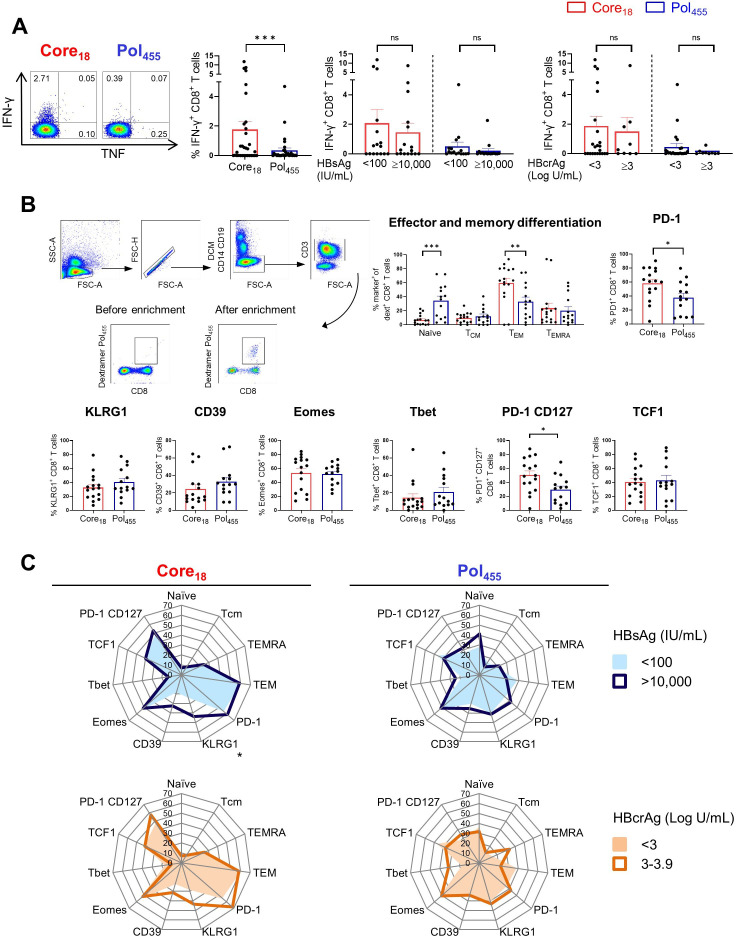
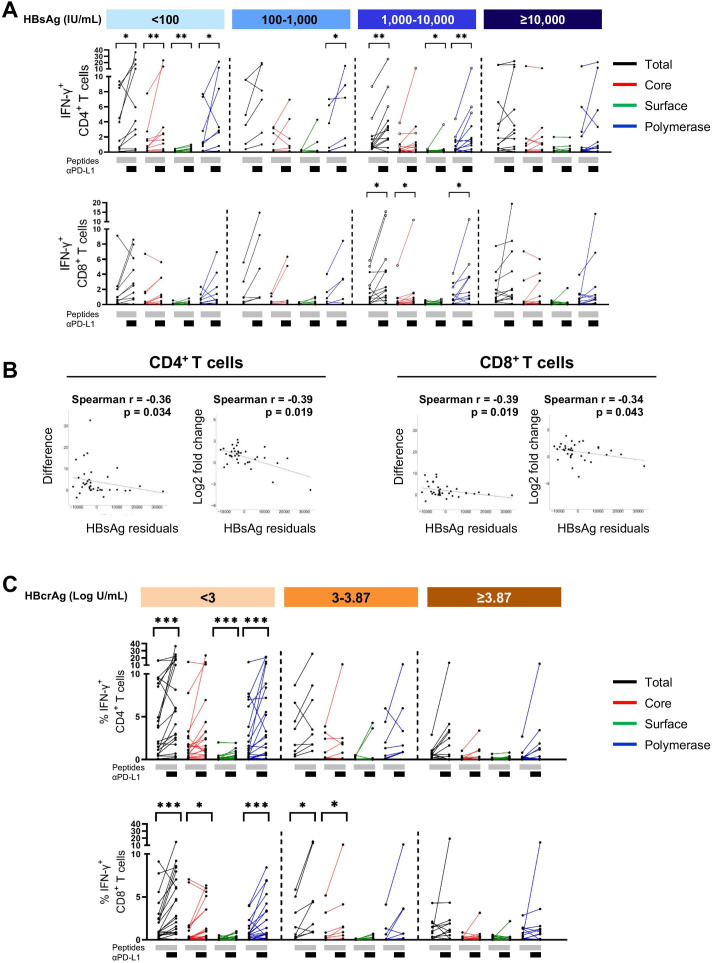
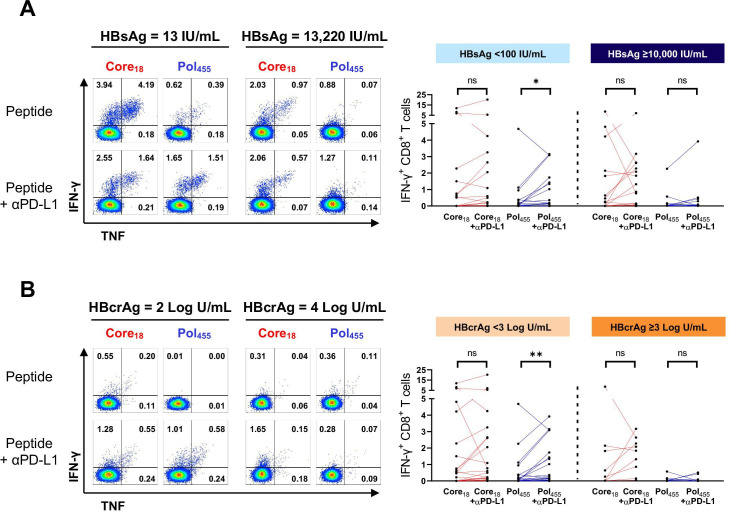
Design: We analysed T cell responses in 92 patients with hepatitis B e antigen negative chronic HBV infection with different HBsAg and HBcrAg levels. Overlapping peptides were used for in vitro response analyses (n=57), and HBV core18-specific and polymerase (pol)455-specific CD8+ T cells were assessed in human leukocyte antigen (HLA)-A*02 patients (n=35). In addition, in vitro responsiveness to anti-programmed cell death-ligand 1 (anti-PD-L1) was investigated.
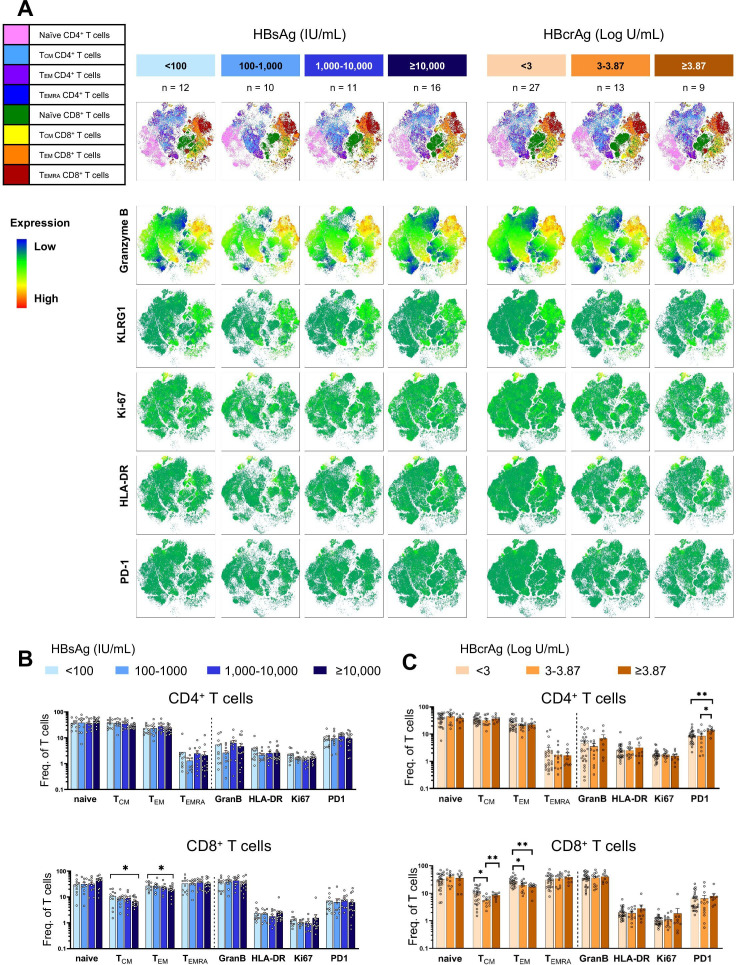
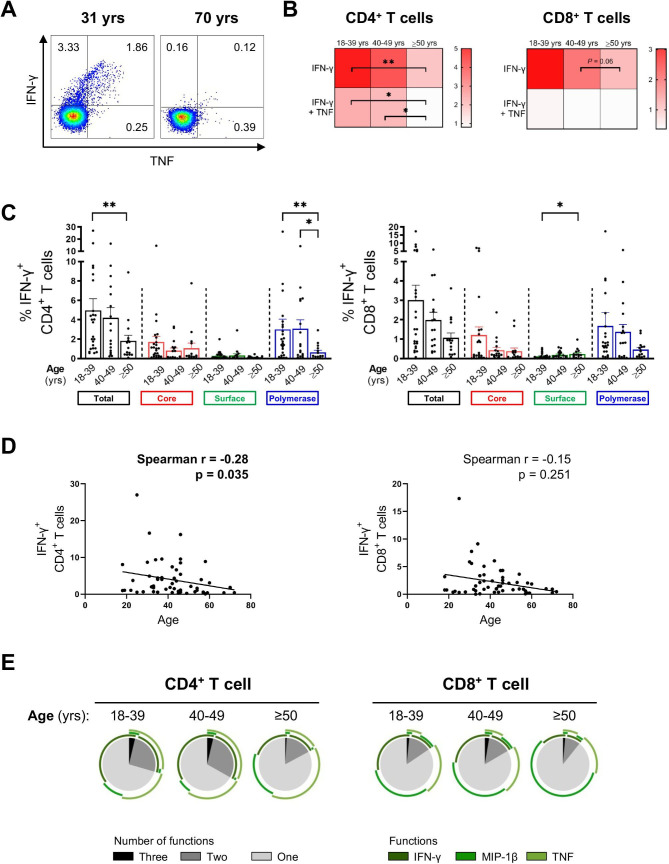
Results: HBV-specific T cell responses were not affected by HBsAg levels, but rather by age and CD4+ T cell responses were highest in patients with low HBcrAg levels. The phenotypes and functionality of HBV core18-specific and pol455-specific CD8+ T cells differed, but HBsAg and HBcrAg levels did not affect their profiles. Blocking with anti-PD-L1 could restore HBV-specific T cells, but the effect was significantly higher in T cells isolated from patients with low HBsAg and in particular low HBcrAg.
Conclusion: Our data suggest that age and HBcrAg rather than HBsAg, are associated with HBV-specific T cell responses. Finally, very low antigen levels indicated by HBsAg and in particular HBcrAg may influence T cell response to checkpoint inhibition.
Keywords: T lymphocytes; cellular immunology; chronic hepatitis; hepatitis B; immune response.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
HBV antigens quantity: duration and effect on functional cure.Gut. 2022 Nov;71(11):2149-2151. doi: 10.1136/gutjnl-2021-326258. Epub 2021 Nov 19. Gut. 2022. PMID: 34799373 No abstract available.
References
-
- World Health Organization . Hepatitis B. Available: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b [Accessed 10 Feb 2021].
-
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu, European Association for the Study of the Liver . EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol 2017;67:370–98. 10.1016/j.jhep.2017.03.021 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials