

Identifying early indicators of secondary peritonitis in critically ill patients with cirrhosis
- PMID: 34702902
- PMCID: PMC8548403
- DOI: 10.1038/s41598-021-00629-4
Identifying early indicators of secondary peritonitis in critically ill patients with cirrhosis
Abstract
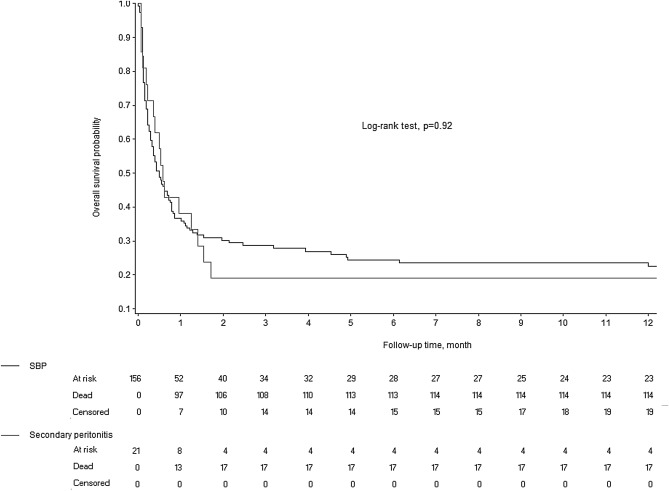
Ascitic fluid infection (AFI) is a life-threatening complication of cirrhosis. We aimed to identify early indicators of secondary peritonitis (SP), which requires emergency surgery, and to describe the outcomes of SP and spontaneous bacterial/fungal peritonitis (SBFP). Adults with cirrhosis and AFI admitted to 16 university or university-affiliated ICUs in France between 2002 and 2017 were studied retrospectively. Cases were identified by searching the hospital databases for relevant ICD-10 codes and hospital charts for AFI. Logistic multivariate regression was performed to identify factors associated with SP. Secondary outcomes were short- and long-term mortality and survivors' functional outcomes. Of 178 included patients (137 men and 41 women; mean age, 58 ± 11 years), 21 (11.8%) had SP, confirmed by surgery in 16 cases and by abdominal computed tomography in 5 cases. Time to diagnosis exceeded 24 h in 7/21 patients with SP. By multivariate analysis, factors independently associated with SP were ascitic leukocyte count > 10,000/mm3 (OR 3.70; 95%CI 1.38-9.85; P = 0.009) and absence of laboratory signs of decompensated cirrhosis (OR 4.53; 95%CI 1.30-15.68; P = 0.017). The 1-year mortality rates in patients with SBFP and SP were 81.0% and 77.5%, respectively (Log-rank test, P = 0.92). Patients with SP vs. SBFP had no differences in 1-year functional outcomes. This multicenter retrospective study identified two indicators of SP as opposed to SBFP in patients with cirrhosis. Using these indicators may help to provide early surgical treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Procalcitonin and macrophage inflammatory protein-1 beta (MIP-1β) in serum and peritoneal fluid of patients with decompensated cirrhosis and spontaneous bacterial peritonitis.Adv Med Sci. 2014 Mar;59(1):52-6. doi: 10.1016/j.advms.2013.07.006. Epub 2014 Mar 21. Adv Med Sci. 2014. PMID: 24797975
-
[Spontaneous bacterial peritonitis: diagnostic and prognostic aspects].Schweiz Med Wochenschr. 1995 Dec 9;125(49):2379-86. Schweiz Med Wochenschr. 1995. PMID: 8848698 German.
-
Prevalence of spontaneous bacterial peritonitis.J Assoc Physicians India. 1992 Apr;40(4):236-8. J Assoc Physicians India. 1992. PMID: 1452529
-
Spontaneous fungal peritonitis: Epidemiology, current evidence and future prospective.World J Gastroenterol. 2016 Sep 14;22(34):7742-7. doi: 10.3748/wjg.v22.i34.7742. World J Gastroenterol. 2016. PMID: 27678356 Free PMC article. Review.
-
Spontaneous bacterial peritonitis.Dis Mon. 1985 Sep;31(9):1-48. doi: 10.1016/0011-5029(85)90002-1. Dis Mon. 1985. PMID: 3899555 Review.
Cited by
-
Differentiation of Spontaneous Bacterial Peritonitis from Secondary Peritonitis in Patients with Liver Cirrhosis: Retrospective Multicentre Study.Diagnostics (Basel). 2023 Mar 6;13(5):994. doi: 10.3390/diagnostics13050994. Diagnostics (Basel). 2023. PMID: 36900138 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
