

Diagnostic performance of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in anorectal melanoma
- PMID: 34703388
- PMCID: PMC8488889
- DOI: 10.4103/wjnm.WJNM_116_20
Diagnostic performance of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in anorectal melanoma
Abstract
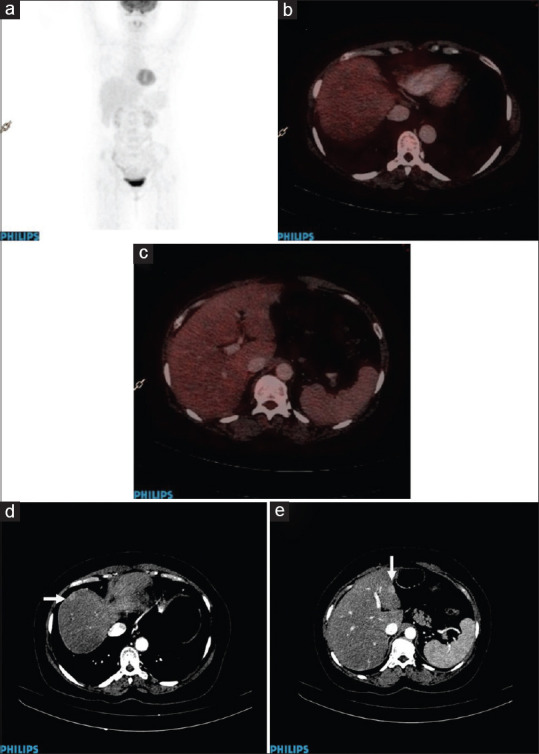
To evaluate the diagnostic role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) in initial staging and restaging of anorectal melanoma. This was a single-institution, retrospective observational study; patients for initial staging and with clinical or radiological suspicion of disease recurrence referred for PET/CT between January 2006 and December 2015 were included in the study. Diagnostic performance of PET/CT was evaluated for baseline staging and disease recurrence. A total of 61 patients who were referred for initial staging were included. PET/CT correctly detected primary lesion in 57 (93.44%) cases, regional nodes in 46 (75.4%) cases, nonregional nodes in 22 (36%) cases, and distant metastases in 25 (41%) cases. The sensitivity (SN); specificity (SP); positive predictive value (PPV); negative predictive value (NPV); and accuracy for primary lesion, regional nodes, nonregional nodes, and distant metastases were 96.6%, 100%, 100%, 50%, and 96.7%; 97.9%, 100%, 100%, 93.3%, and 98.4%; 100%, 100%, 100%, 100%, and 100%; and 100%, 100%, 100%, 100%, and 100%, respectively. A total of 24 patients were included for suspected recurrence/restaging. All the patients were treated previously by surgery, radiotherapy, or chemotherapy. PET/CT detected disease recurrence in 20 (83.3%) patients. Ten patients had recurrence at the primary site, 8 of whom also had distant metastases and 2 had only locoregional metastatic nodes. In the remaining 10 patients, there was no primary site recurrence; however, 2 patients had locoregional nodal and distant metastases and 8 patients had only distant metastases. PET/CT was false negative in 1 patient, which missed liver metastasis. SN, SP, PPV, and NPV of PET/CT was found to be 95%, 100%, 100%, and 75%, respectively, with accuracy of 96%. PET/CT demonstrates overall high diagnostic accuracy in the initial staging and detection of recurrent disease in cases of anorectal melanoma.
Keywords: Accuracy; anorectal; diagnostic; melanoma; positron emission tomography/computed tomography.
Copyright: © 2021 World Journal of Nuclear Medicine.
Conflict of interest statement
There are no conflicts of interest.
Figures




References
LinkOut - more resources
Full Text Sources