

Genicular Artery Embolization for the Treatment of Symptomatic Knee Osteoarthritis
- PMID: 34703964
- PMCID: PMC8542160
- DOI: 10.2106/JBJS.OA.21.00085
Genicular Artery Embolization for the Treatment of Symptomatic Knee Osteoarthritis
Abstract
Genicular artery embolization (GAE) is a novel therapy to treat patients with symptomatic knee osteoarthritis (OA) by reducing synovial arterial hypervascularity. This study evaluates the safety and efficacy of GAE for the treatment of symptomatic knee OA.
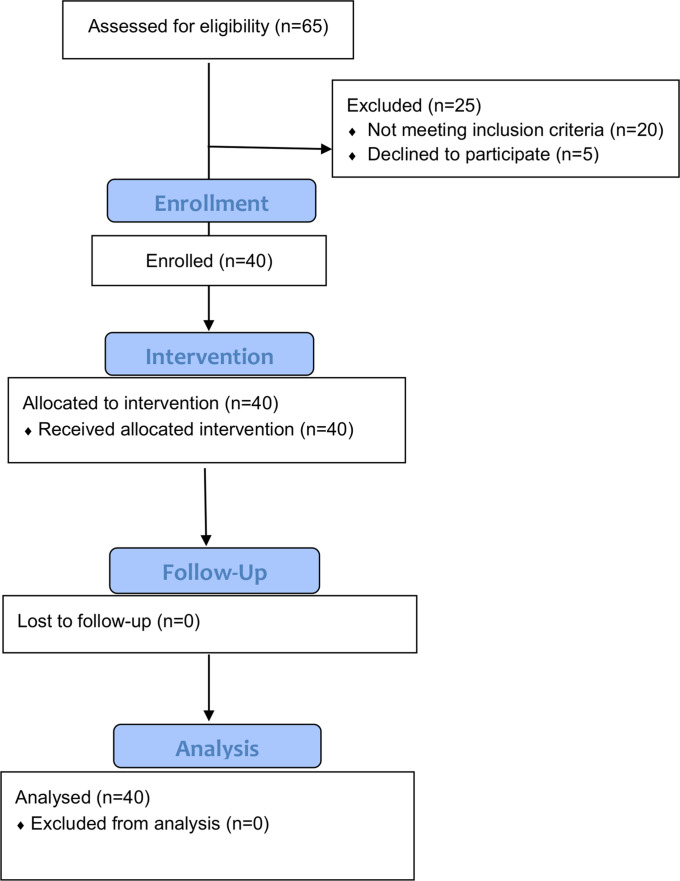
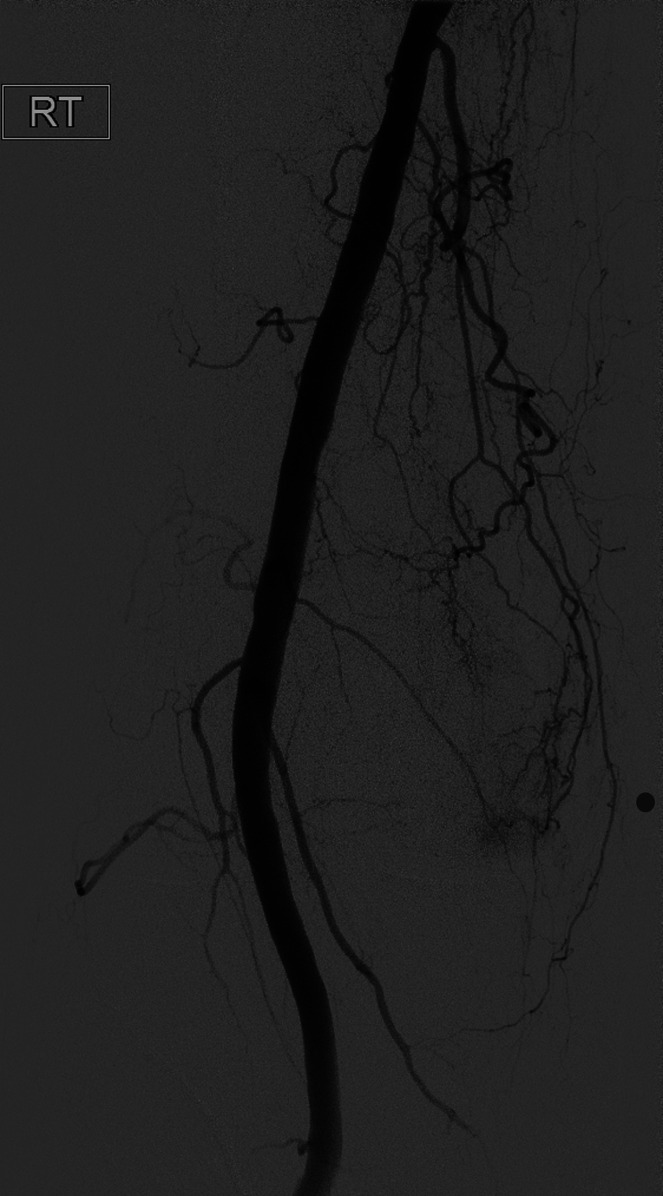
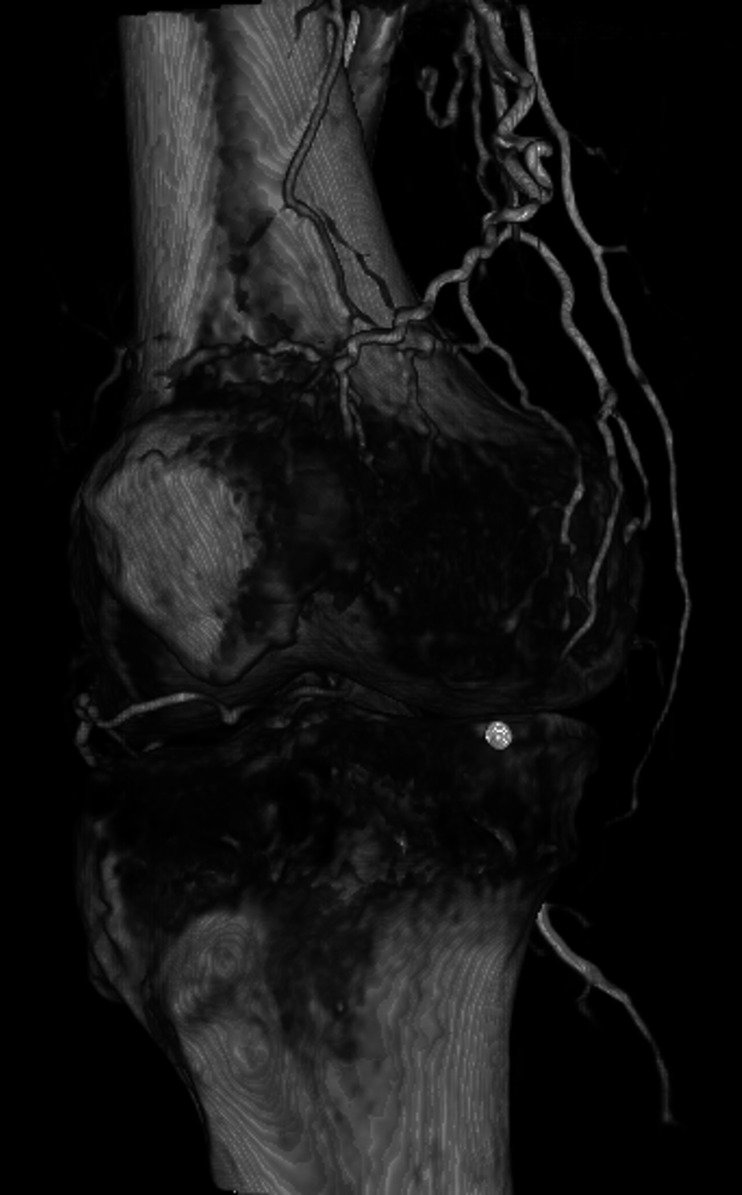
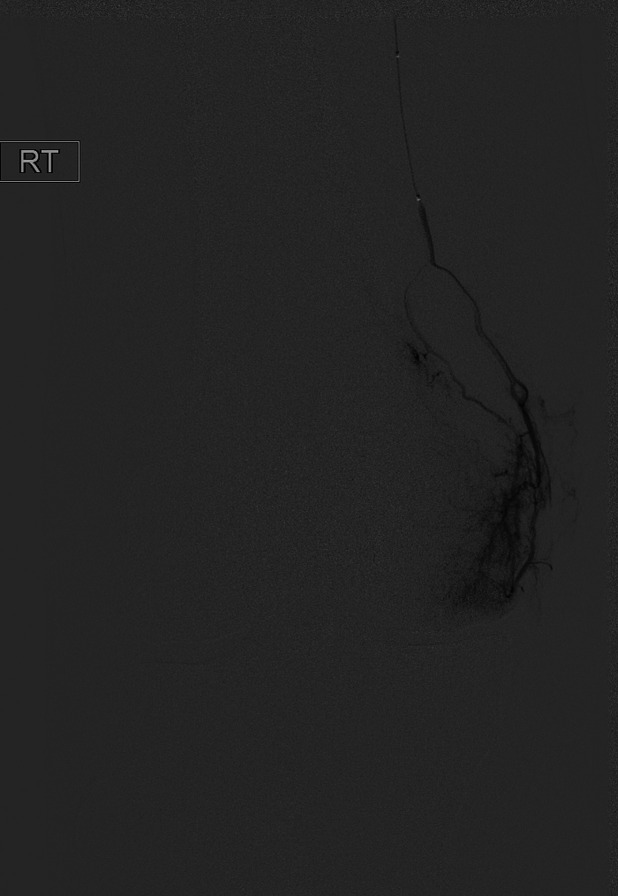
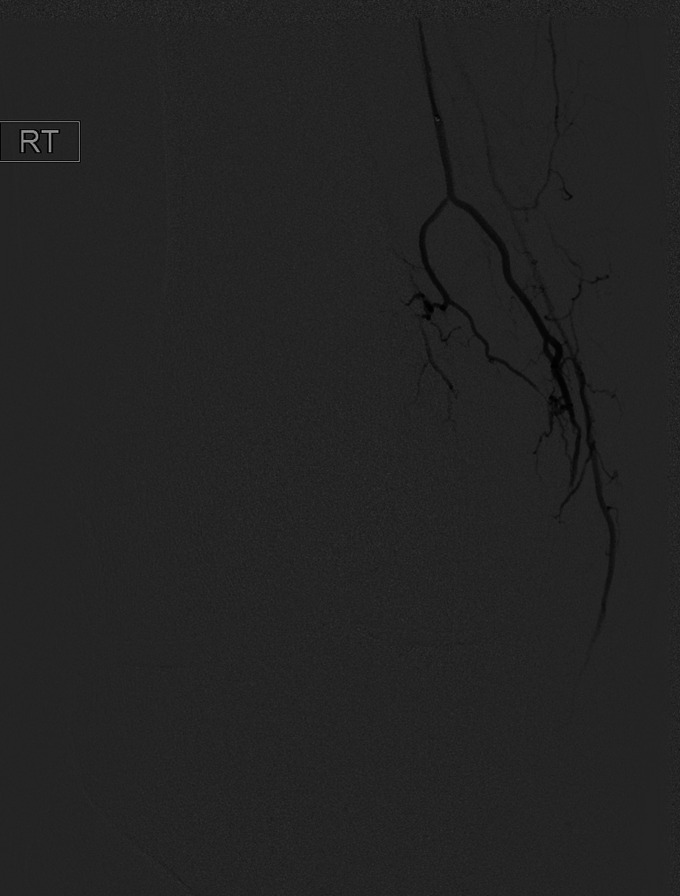
Methods: A prospective, single-center, open-label U.S. Food and Drug Administration-approved investigational device exemption study was conducted. Patients enrolled in the study were 40 to 80 years old, with moderate or severe knee OA (Kellgren-Lawrence grade 2, 3, or 4), who previously had failure of conservative therapy. Baseline pain (visual analog scale [VAS]) and symptom scores (Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC]) were assessed. After femoral arterial access was achieved, GAE of 1, 2, or 3 genicular arteries supplying the location of the subject's pain, as determined by digital subtraction angiography and cone-beam computed tomography, was performed using 100-μm particles. Adverse events and symptoms scores were assessed at 1 week, 1 month, 3 months, 6 months, and 1 year after GAE.
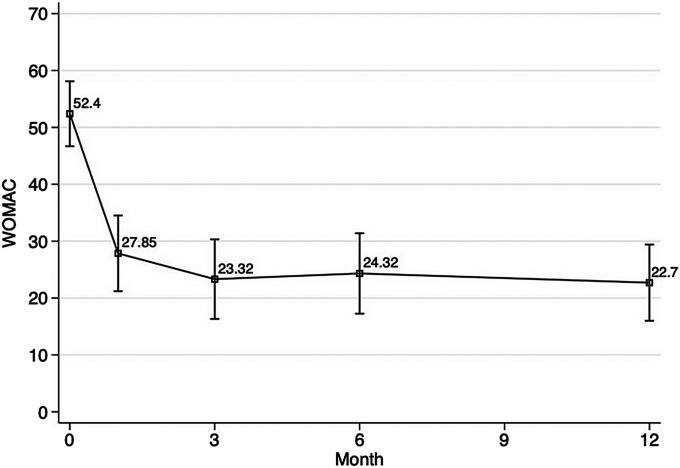
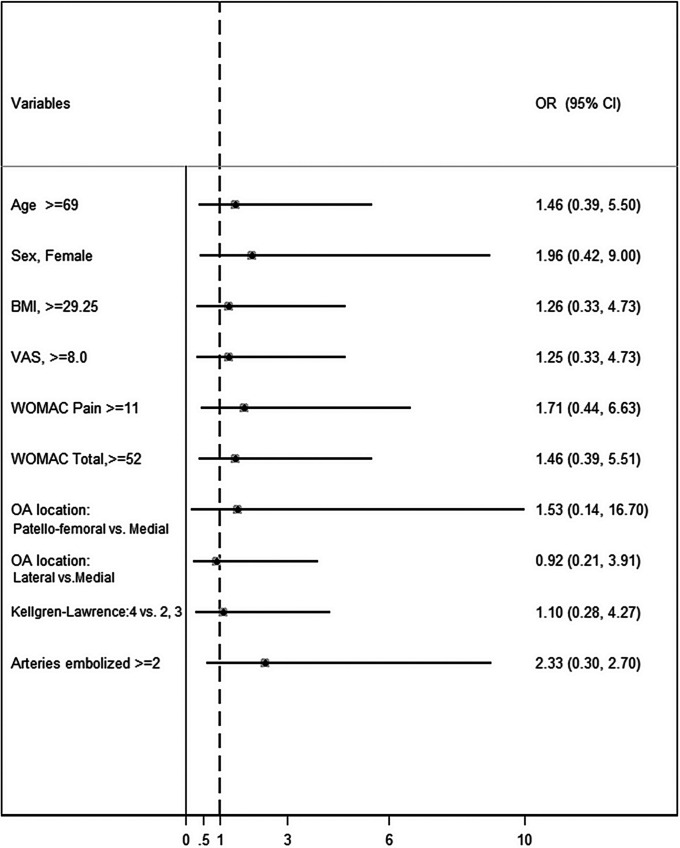
Results: Over a 10-month period, 40 subjects were enrolled. The median age was 69 years (range, 49 to 80 years). The median body mass index was 29 kg/m2 (range, 19 to 44 kg/m2). Knee OA severity was grade 2 in 18% of the patients, grade 3 in 43%, and grade 4 in 40%. Technical success was achieved in 100% of the subjects. Transient skin discoloration and transient mild knee pain after the procedure were common and expected. Treatment-related adverse events included a groin hematoma requiring overnight observation in 1 subject, self-resolving focal skin ulceration in 7 subjects, and an asymptomatic small bone infarct on magnetic resonance imaging at 3 months in 2 subjects. The WOMAC total and VAS pain scores decreased by 61% and 67% at 12 months from a median baseline of 52 (of 96) and 8 (of 10), respectively. Twenty-seven patients (68%) had a reduction of ≥50% in both WOMAC total and VAS pain scores.
Conclusions: This prospective trial demonstrates that GAE is effective and durable in reducing pain symptoms from moderate or severe knee OA that is refractory to other conservative therapy, with an acceptable safety profile.
Level of evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2021 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A326).
Figures


References
-
- Dominick KL, Ahern FM, Gold CH, Heller DA. Health-related quality of life and health service use among older adults with osteoarthritis. Arthritis Rheum. 2004. Jun 15;51(3):326-31. - PubMed
-
- Skou ST, Roos EM, Laursen MB, Rathleff MS, Arendt-Nielsen L, Simonsen O, Rasmussen S. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med. 2015. Oct 22;373(17):1597-606. - PubMed
-
- Delanois RE, Mistry JB, Gwam CU, Mohamed NS, Choksi US, Mont MA. Current Epidemiology of Revision Total Knee Arthroplasty in the United States. J Arthroplasty. 2017. Sep;32(9):2663-8. - PubMed
-
- Sharkey PF, Lichstein PM, Shen C, Tokarski AT, Parvizi J. Why are total knee arthroplasties failing today—has anything changed after 10 years? J Arthroplasty. 2014. Sep;29(9):1774-8. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials