

Cognitive performance in idiopathic intracranial hypertension and relevance of intracranial pressure
- PMID: 34704028
- PMCID: PMC8421706
- DOI: 10.1093/braincomms/fcab202
Cognitive performance in idiopathic intracranial hypertension and relevance of intracranial pressure
Abstract
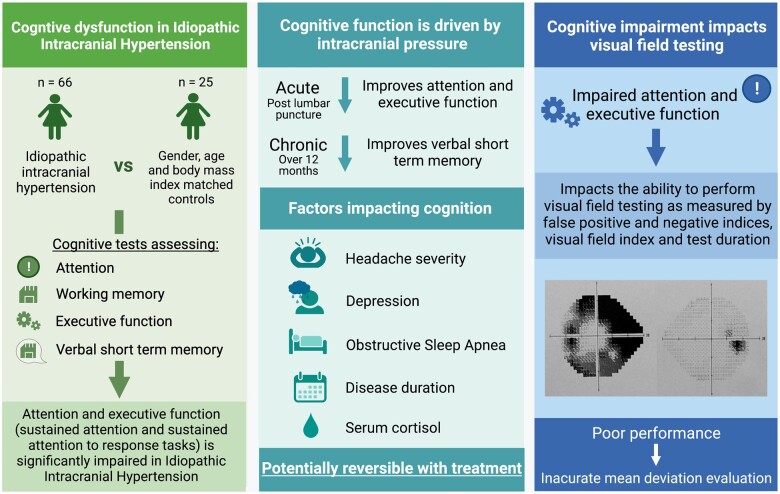
Cognitive impairments have been reported in idiopathic intracranial hypertension; however, evidence supporting these deficits is scarce and contributing factors have not been defined. Using a case-control prospective study, we identified multiple domains of deficiency in a cohort of 66 female adult idiopathic intracranial hypertension patients. We identified significantly impaired attention networks (executive function) and sustained attention compared to a body mass index and age matched control group of 25 healthy female participants. We aimed to investigate how cognitive function changed over time and demonstrated that deficits were not permanent. Participants exhibited improvement in several domains including executive function, sustained attention and verbal short-term memory over 12-month follow-up. Improved cognition over time was associated with reduction in intracranial pressure but not body weight. We then evaluated cognition before and after a lumbar puncture with acute reduction in intracranial pressure and noted significant improvement in sustained attention to response task performance. The impact of comorbidities (headache, depression, adiposity and obstructive sleep apnoea) was also explored. We observed that body mass index and the obesity associated cytokine interleukin-6 (serum and cerebrospinal fluid) were not associated with cognitive performance. Headache severity during cognitive testing, co-morbid depression and markers of obstructive sleep apnoea were adversely associated with cognitive performance. Dysregulation of the cortisol generating enzyme 11β hydroxysteroid dehydrogenase type 1 has been observed in idiopathic intracranial hypertension. Elevated cortisol has been associated with impaired cognition. Here, we utilized liquid chromatography-tandem mass spectrometry for multi-steroid profiling in serum and cerebrospinal fluid in idiopathic intracranial hypertension patients. We noted that reduction in the serum cortisol:cortisone ratio in those undergoing bariatric surgery at 12 months was associated with improving verbal working memory. The clinical relevance of cognitive deficits was noted in their significant association with impaired reliability to perform visual field tests, the cornerstone of monitoring vision in idiopathic intracranial hypertension. Our findings propose that cognitive impairment should be accepted as a clinical manifestation of idiopathic intracranial hypertension and impairs the ability to perform visual field testing reliably. Importantly, cognitive deficits can improve over time and with reduction of intracranial pressure. Treating comorbid depression, obstructive sleep apnoea and headache could improve cognitive performance in idiopathic intracranial hypertension.
Keywords: cognition; headache; idiopathic intracranial hypertension; intracranial pressure; visual field.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources