

Association of Age With the Diagnostic Value of Coronary Artery Calcium Score for Ruling Out Coronary Stenosis in Symptomatic Patients
- PMID: 34705022
- PMCID: PMC8552116
- DOI: 10.1001/jamacardio.2021.4406
Association of Age With the Diagnostic Value of Coronary Artery Calcium Score for Ruling Out Coronary Stenosis in Symptomatic Patients
Abstract
Importance: The diagnostic value is unclear of a 0 coronary artery calcium (CAC) score to rule out obstructive coronary artery disease (CAD) and near-term clinical events across different age groups.
Objective: To assess the diagnostic value of a CAC score of 0 for reducing the likelihood of obstructive CAD and to assess the implications of such a CAC score and obstructive CAD across different age groups.
Design, setting, and participants: This cohort study obtained data from the Western Denmark Heart Registry and had a median follow-up time of 4.3 years. Included patients were aged 18 years or older who underwent computed tomography angiography (CTA) between January 1, 2008, and December 31, 2017, because of symptoms that were suggestive of CAD. Data analysis was performed from April 5 to July 7, 2021.
Exposures: Obstructive CAD, which was defined as 50% or more luminal stenosis.
Main outcomes and measures: Proportion of individuals with obstructive CAD who had a CAC score of 0. Risk-adjusted diagnostic likelihood ratios were used to assess the diagnostic value of a CAC score of 0 for reducing the likelihood of obstructive CAD beyond clinical variables. Risk factors associated with myocardial infarction and death were estimated.
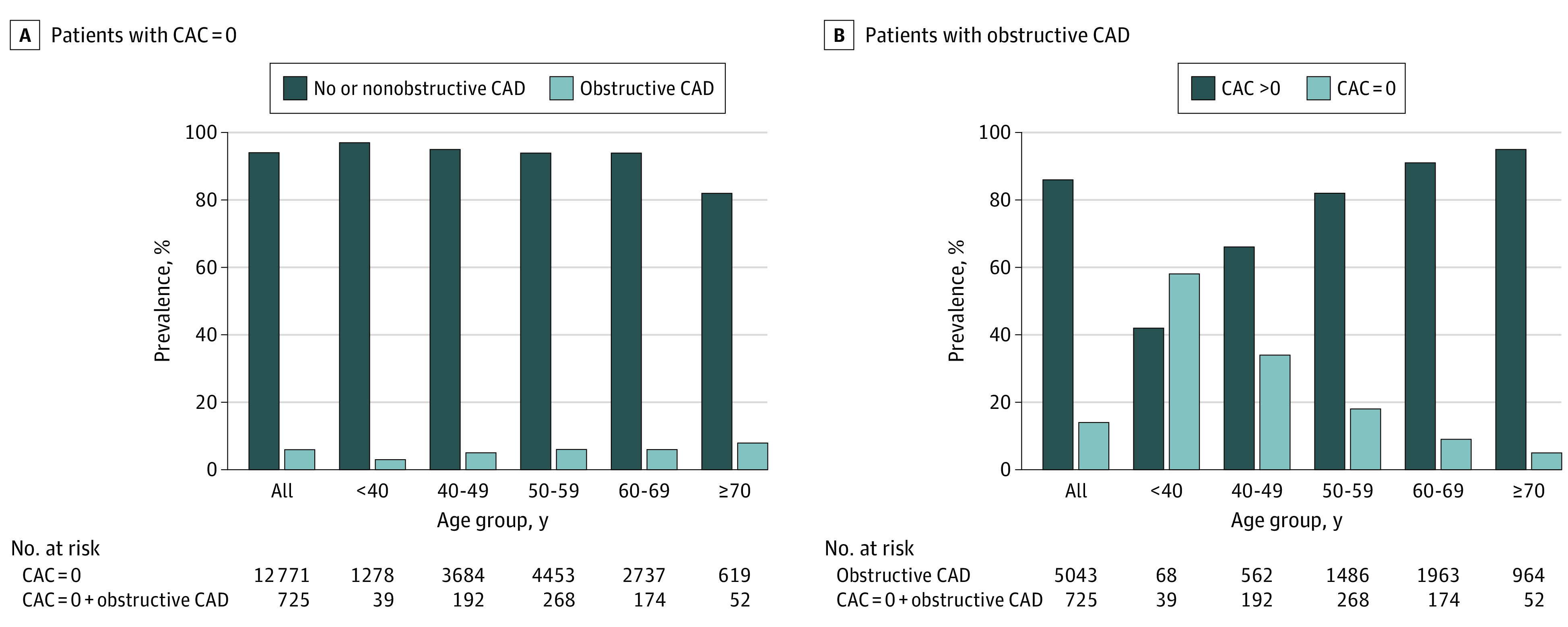
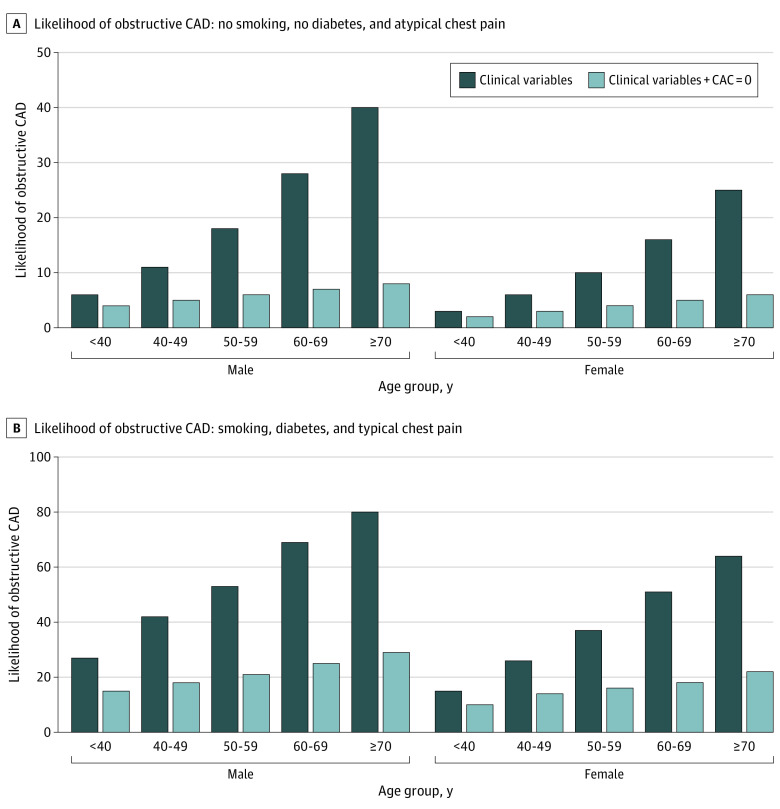
Results: A total of 23 759 symptomatic patients, of whom 12 771 (54%) had a CAC score of 0, were included. This cohort had a median (IQR) age of 58 (49-65) years and was primarily composed of women (13 160 [55%]). Overall, the prevalence of obstructive CAD was relatively low across all age groups, ranging from 3% (39 of 1278 patients) in those who were younger than 40 years to 8% (52 of 619) among those who were 70 years or older. In patients with obstructive CAD, 14% (725 of 5043) had a CAC score of 0, and the prevalence varied across age groups from 58% (39 of 68) among those who were younger than 40 years, 34% (192 of 562) among those aged 40 to 49 years, 18% (268 of 1486) among those aged 50 to 59 years, 9% (174 of 1963) among those aged 60 to 69 years, to 5% (52 of 964) among those who were 70 years or older. The added diagnostic value of a CAC score of 0 decreased at a younger age, with a risk factor-adjusted diagnostic likelihood ratio of a CAC score of 0 ranging from 0.68 (approximately 32% lower likelihood of obstructive CAD than expected) in those who were younger than 40 years to 0.18 (approximately 82% lower likelihood than expected) in those who were 70 years or older. The presence of obstructive vs nonobstructive CAD among those with a CAC score of 0 was associated with a multivariable adjusted hazard ratio of 1.51 (95% CI, 0.98-2.33) for myocardial infarction and all-cause death; however, this hazard ratio varied from 1.80 (95% CI, 1.02-3.19) in those who were younger than 60 years to 1.24 (95% CI, 0.64-2.39) in those who were 60 years or older.
Conclusions and relevance: This cohort study found that the diagnostic value of a CAC score of 0 to rule out obstructive CAD beyond clinical variables was dependent on age, with the added diagnostic value being smaller for younger patients. In symptomatic patients who were younger than 60 years, a sizable proportion of obstructive CAD occurred among those without CAC and was associated with an increased risk of myocardial infarction and all-cause death.
Conflict of interest statement
Figures
Comment in
-
The Potential and Pitfalls of Coronary Artery Calcium Scoring.JAMA Cardiol. 2022 Jan 1;7(1):11-12. doi: 10.1001/jamacardio.2021.4413. JAMA Cardiol. 2022. PMID: 34705021 No abstract available.
-
The "Power of Zero" in Younger Patients-A Glass Half Empty or a Glass Half Full?-Reply.JAMA Cardiol. 2022 Jul 1;7(7):774. doi: 10.1001/jamacardio.2022.0981. JAMA Cardiol. 2022. PMID: 35583883 No abstract available.
-
The "Power of Zero" in Younger Patients-A Glass Half Empty or a Glass Half Full?JAMA Cardiol. 2022 Jul 1;7(7):773-774. doi: 10.1001/jamacardio.2022.0978. JAMA Cardiol. 2022. PMID: 35583888 No abstract available.
References
-
- Blaha MJ, Cainzos-Achirica M, Greenland P, et al. . Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849-858. doi:10.1161/CIRCULATIONAHA.115.018524 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
