

18F-Fludeoxyglucose-Positron Emission Tomography/Computed Tomography and Laparoscopy for Staging of Locally Advanced Gastric Cancer: A Multicenter Prospective Dutch Cohort Study (PLASTIC)
- PMID: 34705049
- PMCID: PMC8552113
- DOI: 10.1001/jamasurg.2021.5340
18F-Fludeoxyglucose-Positron Emission Tomography/Computed Tomography and Laparoscopy for Staging of Locally Advanced Gastric Cancer: A Multicenter Prospective Dutch Cohort Study (PLASTIC)
Abstract
Importance: The optimal staging for gastric cancer remains a matter of debate.
Objective: To evaluate the value of 18F-fludeoxyglucose-positron emission tomography with computed tomography (FDG-PET/CT) and staging laparoscopy (SL) in addition to initial staging by means of gastroscopy and CT in patients with locally advanced gastric cancer.
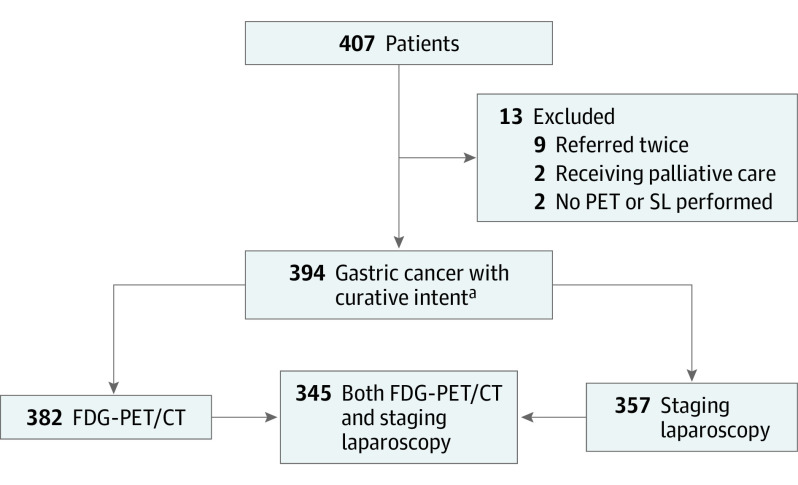
Design, setting, and participants: This multicenter prospective, observational cohort study included 394 patients with locally advanced, clinically curable gastric adenocarcinoma (≥cT3 and/or N+, M0 category based on CT) between August 1, 2017, and February 1, 2020.
Exposures: All patients underwent an FDG-PET/CT and/or SL in addition to initial staging.
Main outcomes and measures: The primary outcome was the number of patients in whom the intent of treatment changed based on the results of these 2 investigations. Secondary outcomes included diagnostic performance, number of incidental findings on FDG-PET/CT, morbidity and mortality after SL, and diagnostic delay.
Results: Of the 394 patients included, 256 (65%) were men and mean (SD) age was 67.6 (10.7) years. A total of 382 patients underwent FDG-PET/CT and 357 underwent SL. Treatment intent changed from curative to palliative in 65 patients (16%) based on the additional FDG-PET/CT and SL findings. FDG-PET/CT detected distant metastases in 12 patients (3%), and SL detected peritoneal or locally nonresectable disease in 73 patients (19%), with an overlap of 7 patients (2%). FDG-PET/CT had a sensitivity of 33% (95% CI, 17%-53%) and specificity of 97% (95% CI, 94%-99%) in detecting distant metastases. Secondary findings on FDG/PET were found in 83 of 382 patients (22%), which led to additional examinations in 65 of 394 patients (16%). Staging laparoscopy resulted in a complication requiring reintervention in 3 patients (0.8%) without postoperative mortality. The mean (SD) diagnostic delay was 19 (14) days.
Conclusions and relevance: This study's findings suggest an apparently limited additional value of FDG-PET/CT; however, SL added considerably to the staging process of locally advanced gastric cancer by detection of peritoneal and nonresectable disease. Therefore, it may be useful to include SL in guidelines for staging advanced gastric cancer, but not FDG-PET/CT.
Conflict of interest statement
Figures
Comment in
-
Optimal Staging for Gastric Cancer Starts With High-Resolution Computed Tomography.JAMA Surg. 2021 Dec 1;156(12):e215330. doi: 10.1001/jamasurg.2021.5330. Epub 2021 Dec 8. JAMA Surg. 2021. PMID: 34705027 No abstract available.
References
-
- Integraal Kankercentrum Nederland . Diagnostiek, behandeling en follow-up van het maagcarcinoom 2016. Published 2017. Accessed September 20, 2021. https://richtlijnendatabase.nl/gerelateerde_documenten/f/16316/IKNL%20ri...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
