

Association between cardiometabolic disease multimorbidity and all-cause mortality in 2 million women and men registered in UK general practices
- PMID: 34706724
- PMCID: PMC8555122
- DOI: 10.1186/s12916-021-02126-x
Association between cardiometabolic disease multimorbidity and all-cause mortality in 2 million women and men registered in UK general practices
Abstract
Background: Myocardial infarction (MI), stroke and diabetes share underlying risk factors and commonalities in clinical management. We examined if their combined impact on mortality is proportional, amplified or less than the expected risk separately of each disease and whether the excess risk is explained by their associated comorbidities.
Methods: Using large-scale electronic health records, we identified 2,007,731 eligible patients (51% women) and registered with general practices in the UK and extracted clinical information including diagnosis of myocardial infarction (MI), stroke, diabetes and 53 other long-term conditions before 2005 (study baseline). We used Cox regression to determine the risk of all-cause mortality with age as the underlying time variable and tested for excess risk due to interaction between cardiometabolic conditions.
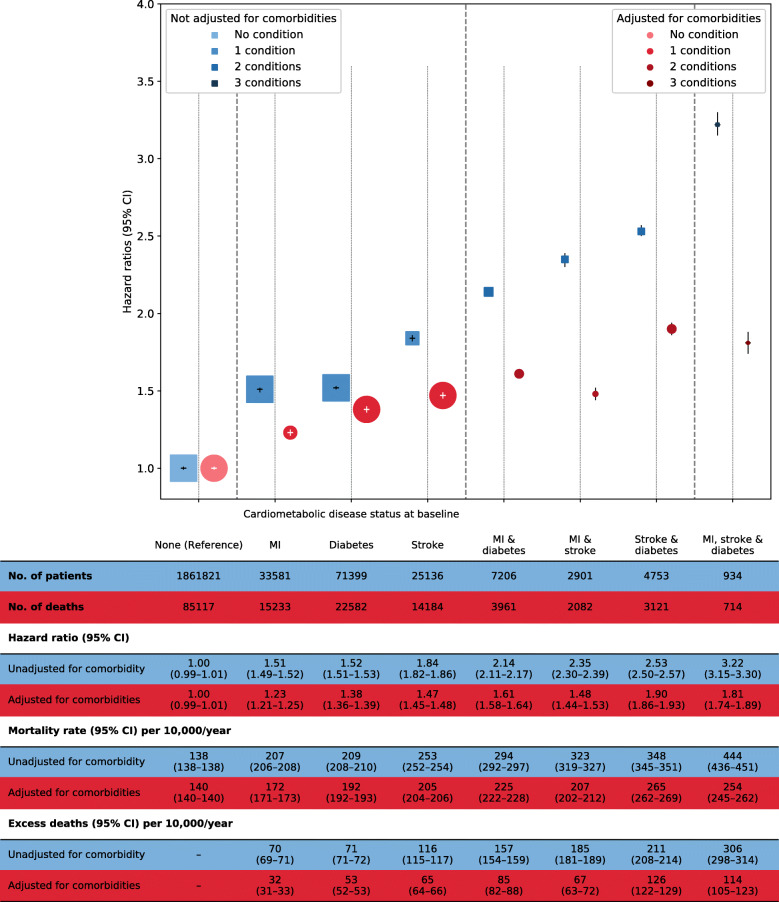
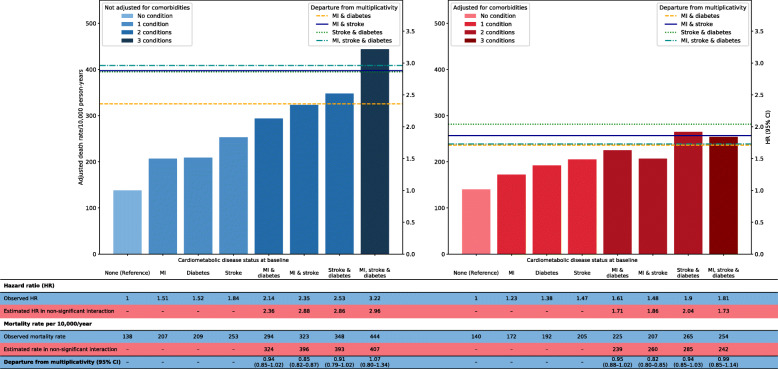
Results: At baseline, the mean age was 51 years, and 7% (N = 145,910) have had a cardiometabolic condition. After a 7-year mean follow-up, 146,994 died. The sex-adjusted hazard ratios (HR) (95% confidence interval [CI]) of all-cause mortality by baseline disease status, compared to those without cardiometabolic disease, were MI = 1.51 (1.49-1.52), diabetes = 1.52 (1.51-1.53), stroke = 1.84 (1.82-1.86), MI and diabetes = 2.14 (2.11-2.17), MI and stroke = 2.35 (2.30-2.39), diabetes and stroke = 2.53 (2.50-2.57) and all three = 3.22 (3.15-3.30). Adjusting for other concurrent comorbidities attenuated these estimates, including the risk associated with having all three conditions (HR = 1.81 [95% CI 1.74-1.89]). Excess risks due to interaction between cardiometabolic conditions, particularly when all three conditions were present, were not significantly greater than expected from the individual disease effects.
Conclusion: Myocardial infarction, stroke and diabetes were associated with excess mortality, without evidence of any amplification of risk in people with all three diseases. The presence of other comorbidities substantially contributed to the excess mortality risks associated with cardiometabolic disease multimorbidity.
Keywords: Diabetes; Electronic health records; Mortality; Multimorbidity; Myocardial infarction; Stroke.
© 2021. The Author(s).
Conflict of interest statement
KR, DC and JT have received support from the NIHR, British Heart Foundation, Oxford Martin School, Rhodes Trust or Clarendon Fund; other authors have no competing interest to declare. Funding organizations had no role in the design or conduct of the study; data collection, management, analysis and interpretation; and manuscript preparation, review or approval to submit for publication.
Figures
References
-
- The Academy of Medical Sciences. Multimorbidity: a priority for global health research: The Academy of Medical Sciences; 2018.
-
- Tran J, Norton R, Conrad N, Rahimian F, Canoy D, Nazarzadeh M, Rahimi K. Patterns and temporal trends of comorbidity among adult patients with incident cardiovascular disease in the UK between 2000 and 2014: a population-based cohort study. PLoS Med. 2018;15(3):e1002513. doi: 10.1371/journal.pmed.1002513. - DOI - PMC - PubMed
-
- Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2(8):634–647. doi: 10.1016/S2213-8587(14)70102-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
