

Conversion from Calcineurin Inhibitor- to Belatacept-Based Maintenance Immunosuppression in Renal Transplant Recipients: A Randomized Phase 3b Trial
- PMID: 34706967
- PMCID: PMC8638403
- DOI: 10.1681/ASN.2021050628
Conversion from Calcineurin Inhibitor- to Belatacept-Based Maintenance Immunosuppression in Renal Transplant Recipients: A Randomized Phase 3b Trial
Abstract
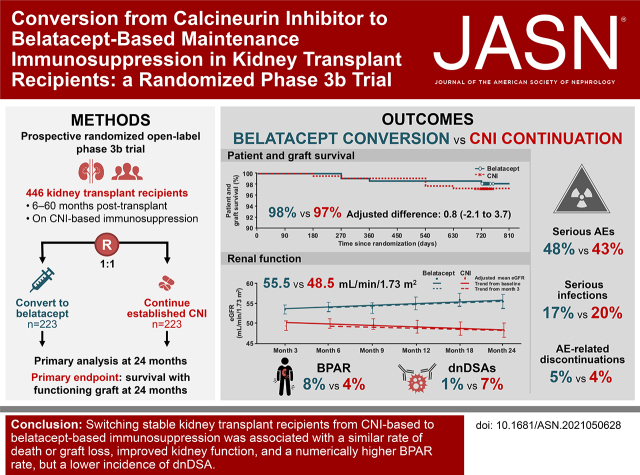
Background: Calcineurin inhibitors (CNIs) are standard of care after kidney transplantation, but they are associated with nephrotoxicity and reduced long-term graft survival. Belatacept, a selective T cell costimulation blocker, is approved for the prophylaxis of kidney transplant rejection. This phase 3 trial evaluated the efficacy and safety of conversion from CNI-based to belatacept-based maintenance immunosuppression in kidney transplant recipients.
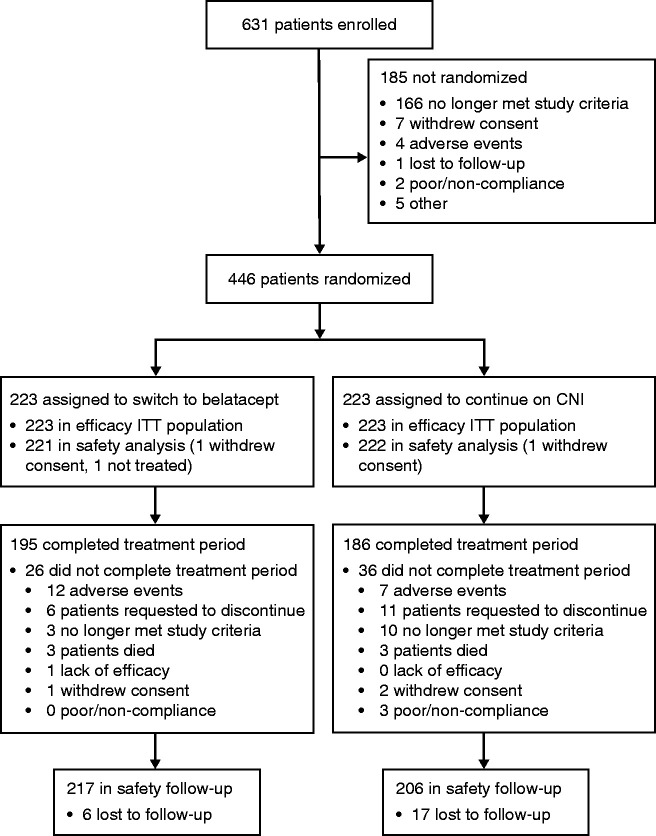
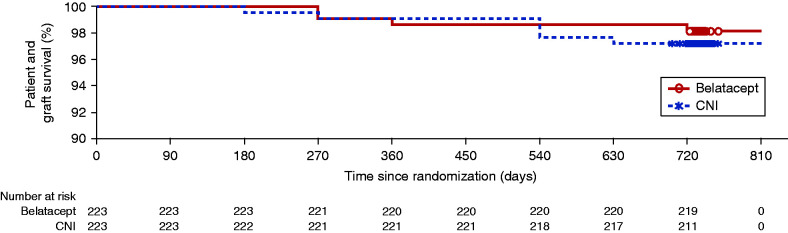
Methods: Stable adult kidney transplant recipients 6-60 months post-transplantation under CNI-based immunosuppression were randomized (1:1) to switch to belatacept or continue treatment with their established CNI. The primary end point was the percentage of patients surviving with a functioning graft at 24 months.
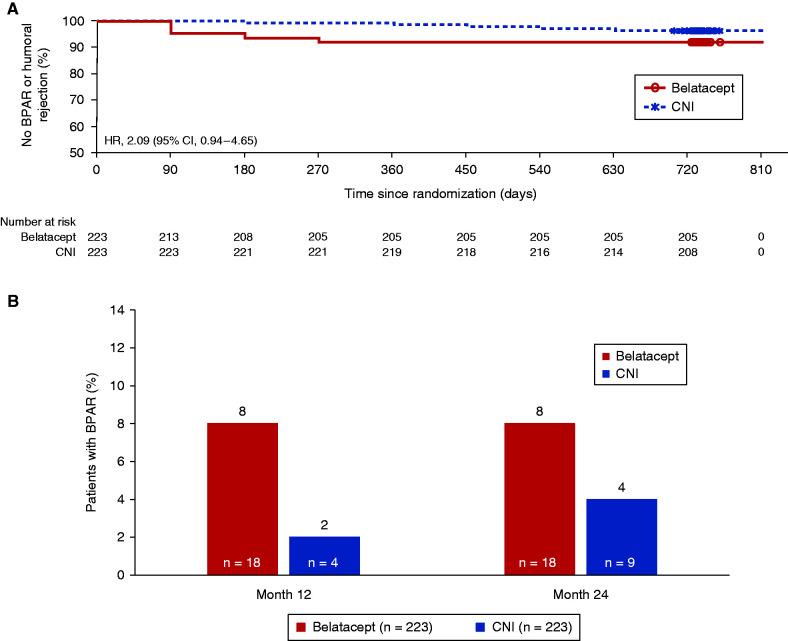
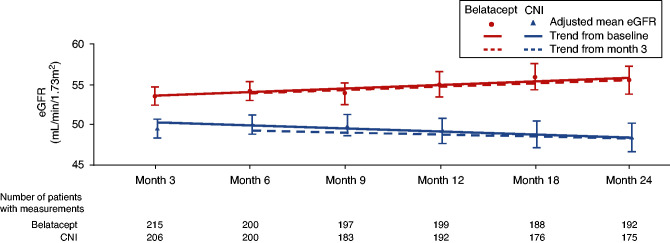
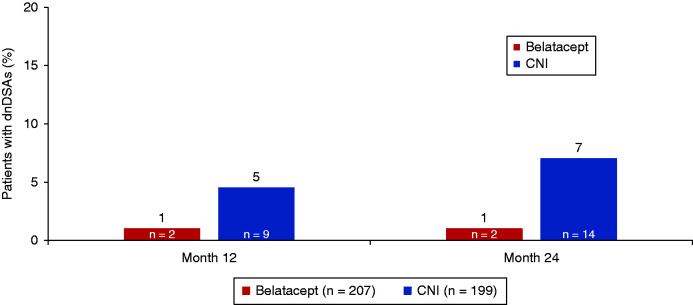
Results: Overall, 446 renal transplant recipients were randomized to belatacept conversion ( n =223) or CNI continuation ( n =223). The 24-month rates of survival with graft function were 98% and 97% in the belatacept and CNI groups, respectively (adjusted difference, 0.8; 95.1% CI, -2.1 to 3.7). In the belatacept conversion versus CNI continuation groups, 8% versus 4% of patients experienced biopsy-proven acute rejection (BPAR), respectively, and 1% versus 7% developed de novo donor-specific antibodies (dnDSAs), respectively. The 24-month eGFR was higher with belatacept (55.5 versus 48.5 ml/min per 1.73 m 2 with CNI). Both groups had similar rates of serious adverse events, infections, and discontinuations, with no unexpected adverse events. One patient in the belatacept group had post-transplant lymphoproliferative disorder.
Conclusions: Switching stable renal transplant recipients from CNI-based to belatacept-based immunosuppression was associated with a similar rate of death or graft loss, improved renal function, and a numerically higher BPAR rate but a lower incidence of dnDSA.Clinical Trial registry name and registration number: A Study in Maintenance Kidney Transplant Recipients Following Conversion to Nulojix® (Belatacept)-Based, NCT01820572.
Copyright © 2021 by the American Society of Nephrology.
Figures
Comment in
-
It Is Time for Patient-Reported Outcome Measures to Be Included in the Approval Process for Solid Organ Transplant Medications.J Am Soc Nephrol. 2021 Dec 1;32(12):2984-2986. doi: 10.1681/ASN.2021081136. Epub 2021 Dec 1. J Am Soc Nephrol. 2021. PMID: 36734821 Free PMC article. No abstract available.
References
-
- Azzi JR, Sayegh MH, Mallat SG: Calcineurin inhibitors: 40 years later, can’t live without …. J Immunol 191: 5785–5791, 2013 - PubMed
-
- Malvezzi P, Rostaing L: The safety of calcineurin inhibitors for kidney-transplant patients. Expert Opin Drug Saf 14: 1531–1546, 2015 - PubMed
-
- Everly MJ, Rebellato LM, Haisch CE, Ozawa M, Parker K, Briley KP, et al. : Incidence and impact of de novo donor-specific alloantibody in primary renal allografts. Transplantation 95: 410–417, 2013 - PubMed
-
- Sawinski D, Trofe-Clark J, Leas B, Uhl S, Tuteja S, Kaczmarek JL, et al. : Calcineurin inhibitor minimization, conversion, withdrawal, and avoidance strategies in renal transplantation: A systematic review and meta-analysis. Am J Transplant 16: 2117–2138, 2016 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
