

Small Fiber Neuropathy Incidence, Prevalence, Longitudinal Impairments, and Disability
- PMID: 34706972
- PMCID: PMC8641968
- DOI: 10.1212/WNL.0000000000012894
Small Fiber Neuropathy Incidence, Prevalence, Longitudinal Impairments, and Disability
Abstract
Background and objectives: There are limited population-based data on small fiber neuropathy (SFN). We wished to determine SFN incidence, prevalence, comorbid conditions, longitudinal impairments, and disabilities.
Methods: Test-confirmed patients with SFN in Olmsted, Minnesota, and adjacent counties were compared 3:1 to matched controls (January 1, 1998-December 31, 2017).
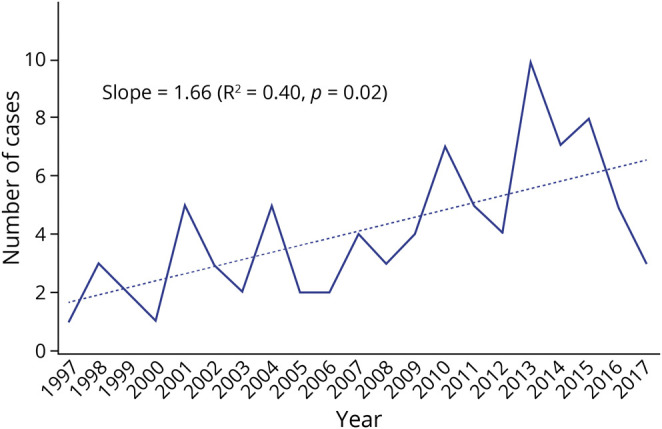
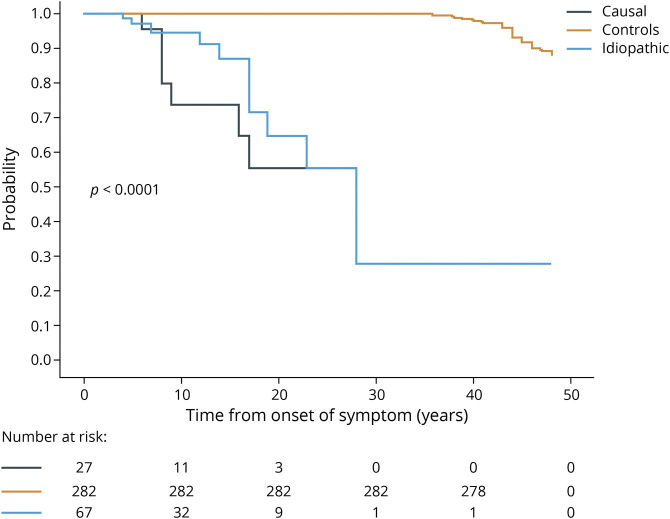
Results: Ninety-four patients with SFN were identified, with an incidence of 1.3/100,000/y that increased over the study period and a prevalence of 13.3 per 100,000. Average follow-up was 6.1 years (0.7-43 years), and mean onset age was 54 years (range 14-83 years). Female sex (67%), obesity (body mass index mean 30.4 vs 28.5 kg/m2), insomnia (86% vs 54%), analgesic-opioid prescriptions (72% vs 46%), hypertriglyceridemia (180 mg/dL mean vs 147 mg/dL), and diabetes (51% vs 22%, p < 0.001) were more common (odds ratio 3.8-9.0, all p < 0.03). Patients with SFN did not self-identify as disabled with a median modified Rankin Scale score of 1.0 (range 0-6) vs 0.0 (0-6) for controls (p = 0.04). Higher Charlson comorbid conditions (median 6, range 3-9) occurred vs controls (median 3, range 1-9, p < 0.001). Myocardial infarctions occurred in 46% vs 27% of controls (p < 0.0001). Classifications included idiopathic (70%); diabetes (15%); Sjögren disease (2%); AL-amyloid (1%); transthyretin-amyloid (1%); Fabry disease (1%); lupus (1%); postviral (1%); Lewy body (1%), and multifactorial (5%). Foot ulcers occurred in 17, with 71% having diabetes. Large fiber neuropathy developed in 36%, on average 5.3 years (range 0.2-14.3 years) from SFN onset. Median onset Composite Autonomic Severity Score (CASS) was 3 (change per year 0.08, range 0-2.0). Median Neuropathy Impairment Scale (NIS) score was 2 at onset (range 0-8, change per year 1.0, range -7.9 to +23.3). NIS score and CASS change >1 point per year occurred in only AL-amyloid, hereditary transthyretin-amyloid, Fabry, uncontrolled diabetes, and Lewy body. Death after symptom onset was higher in patients with SFN (19%) vs controls (12%, p < 0.001), 50% secondary to diabetes complications.
Discussion: Isolated SFN is uncommon but increasing in incidence. Most patients do not develop major neurologic impairments and disability but have multiple comorbid conditions, including cardiovascular ischemic events, and increased mortality from SFN onsets. Development of large fiber involvements and diabetes are common over time. Targeted testing facilitates interventional therapies for diabetes but also rheumatologic and rare genetic forms.
© 2021 American Academy of Neurology.
Figures
Comment in
-
Causes and Implications of Isolated Small Fiber Neuropathy.Neurology. 2021 Nov 30;97(22):1015-1016. doi: 10.1212/WNL.0000000000012895. Epub 2021 Oct 27. Neurology. 2021. PMID: 34706973 No abstract available.
References
-
- Peters MJ, Bakkers M, Merkies IS, Hoeijmakers JG, van Raak EP, Faber CG. Incidence and prevalence of small-fiber neuropathy: a survey in the Netherlands. Neurology. 2013;81(15):1356-1360. - PubMed
-
- Bakkers M, Faber CG, Hoeijmakers JG, Lauria G, Merkies IS. Small fibers, large impact: quality of life in small-fiber neuropathy. Muscle Nerve. 2014;49(3):329-336. - PubMed
-
- Singer W, Spies JM, McArthur J, et al. Prospective evaluation of somatic and autonomic small fibers in selected autonomic neuropathies. Neurology. 2004;62(4):612-618. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous