

Automated segmentation by deep learning of loose connective tissue fibers to define safe dissection planes in robot-assisted gastrectomy
- PMID: 34707141
- PMCID: PMC8551298
- DOI: 10.1038/s41598-021-00557-3
Automated segmentation by deep learning of loose connective tissue fibers to define safe dissection planes in robot-assisted gastrectomy
Abstract
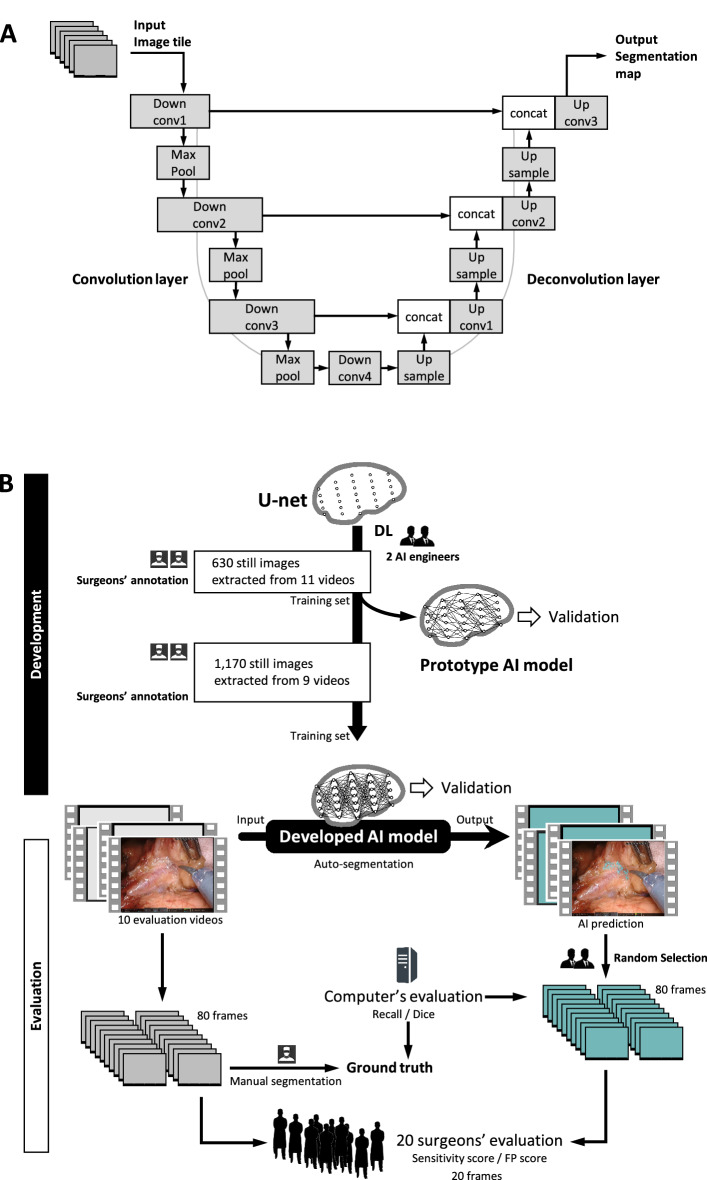
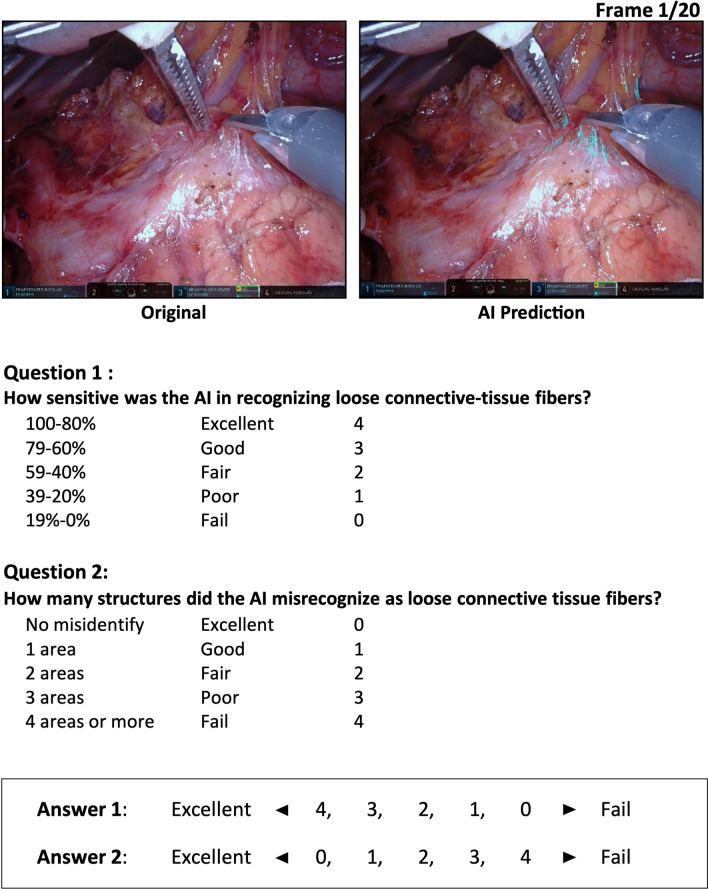
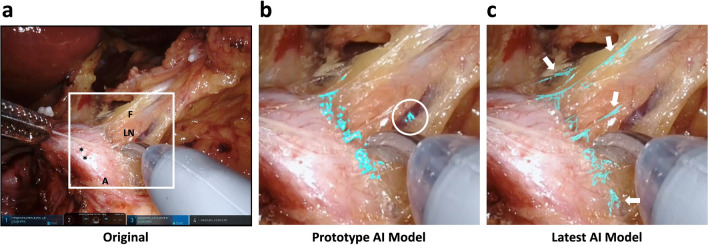
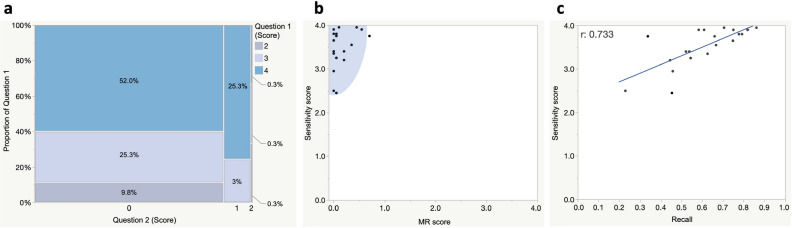
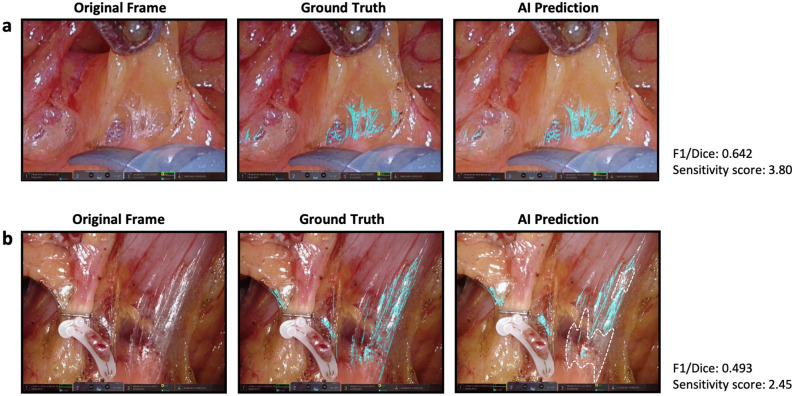
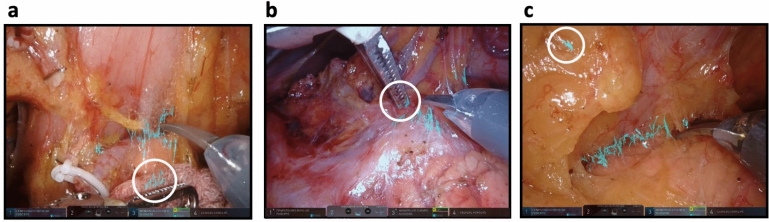
The prediction of anatomical structures within the surgical field by artificial intelligence (AI) is expected to support surgeons' experience and cognitive skills. We aimed to develop a deep-learning model to automatically segment loose connective tissue fibers (LCTFs) that define a safe dissection plane. The annotation was performed on video frames capturing a robot-assisted gastrectomy performed by trained surgeons. A deep-learning model based on U-net was developed to output segmentation results. Twenty randomly sampled frames were provided to evaluate model performance by comparing Recall and F1/Dice scores with a ground truth and with a two-item questionnaire on sensitivity and misrecognition that was completed by 20 surgeons. The model produced high Recall scores (mean 0.606, maximum 0.861). Mean F1/Dice scores reached 0.549 (range 0.335-0.691), showing acceptable spatial overlap of the objects. Surgeon evaluators gave a mean sensitivity score of 3.52 (with 88.0% assigning the highest score of 4; range 2.45-3.95). The mean misrecognition score was a low 0.14 (range 0-0.7), indicating very few acknowledged over-detection failures. Thus, AI can be trained to predict fine, difficult-to-discern anatomical structures at a level convincing to expert surgeons. This technology may help reduce adverse events by determining safe dissection planes.
© 2021. The Author(s).
Conflict of interest statement
Y.K. and N.K. are shareholders of Anaut, Inc. N.K. is a shareholder of Incubit, Inc. E.R. and P.N. are technical staff of Incubit, Inc. The sponsor had no role in the study design, data collection, data analysis, manuscript preparation, or publication decisions. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
