

Predicting and comparing three corrective techniques for sagittal craniosynostosis
- PMID: 34707183
- PMCID: PMC8551239
- DOI: 10.1038/s41598-021-00642-7
Predicting and comparing three corrective techniques for sagittal craniosynostosis
Abstract
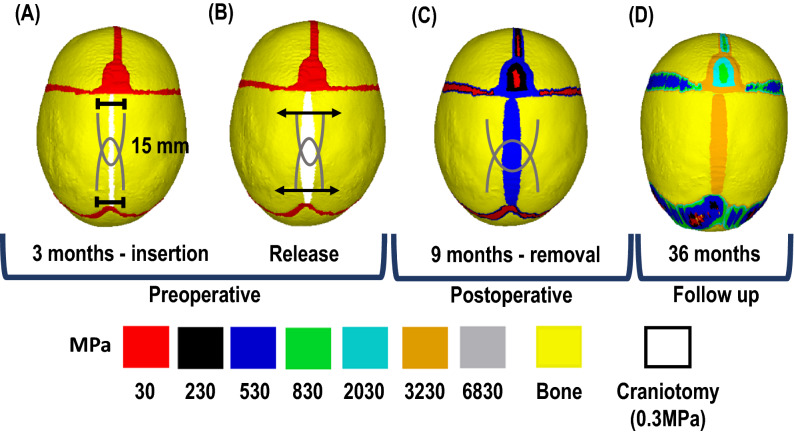
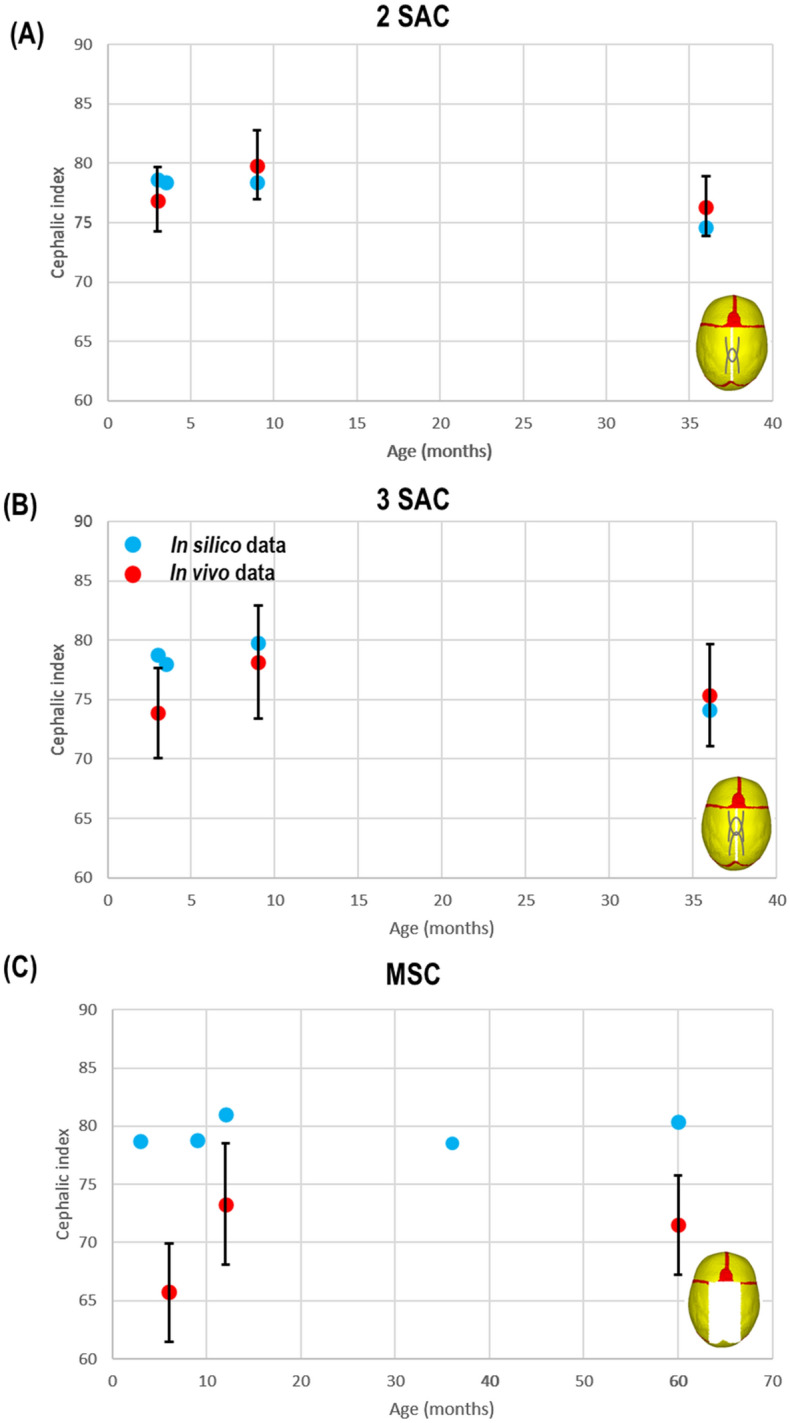
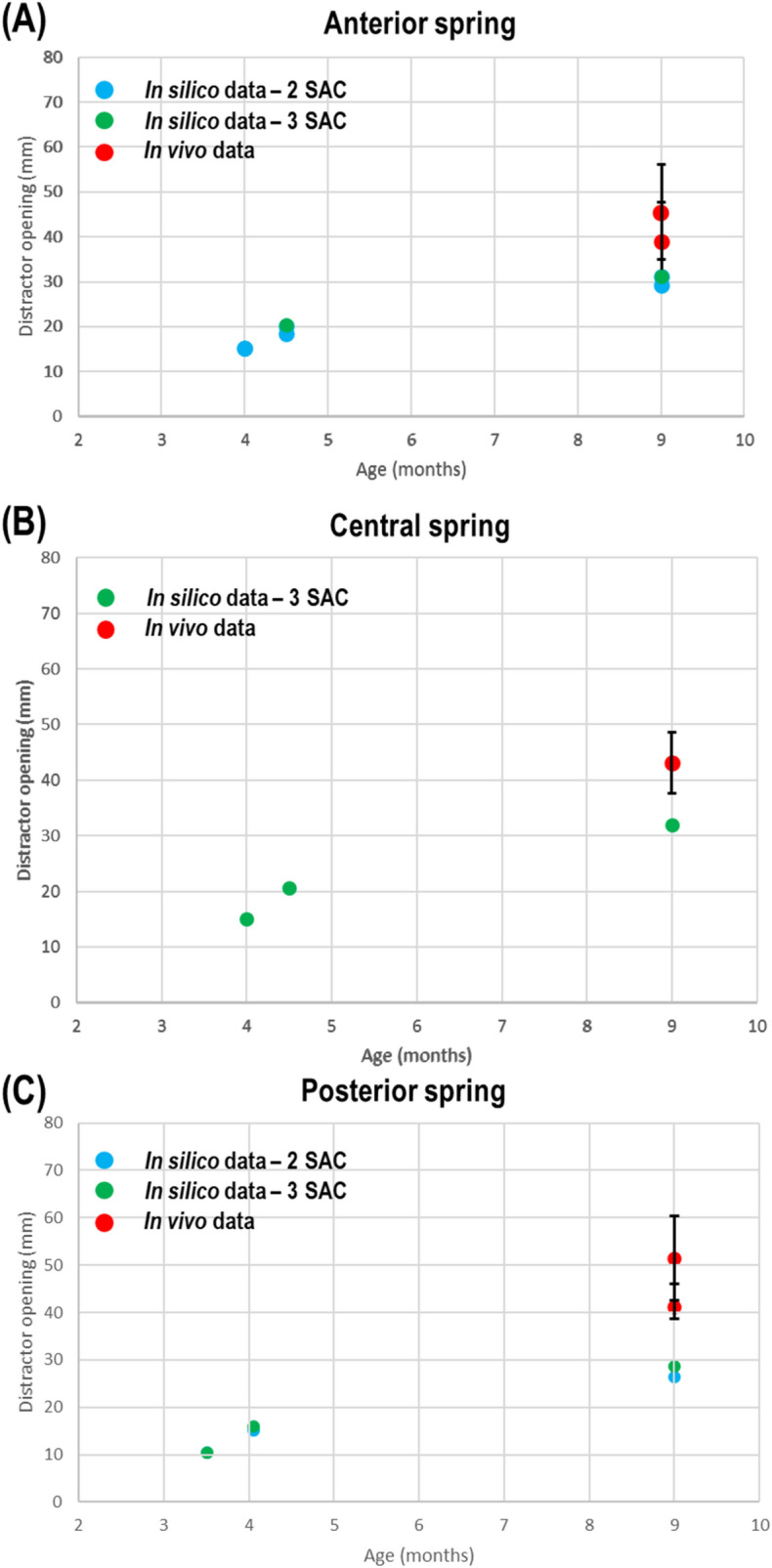
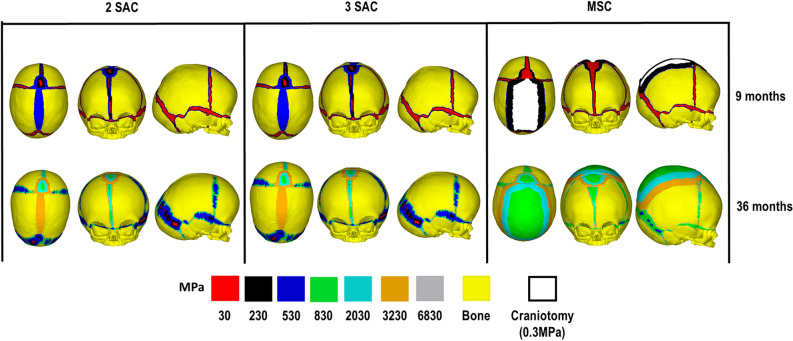
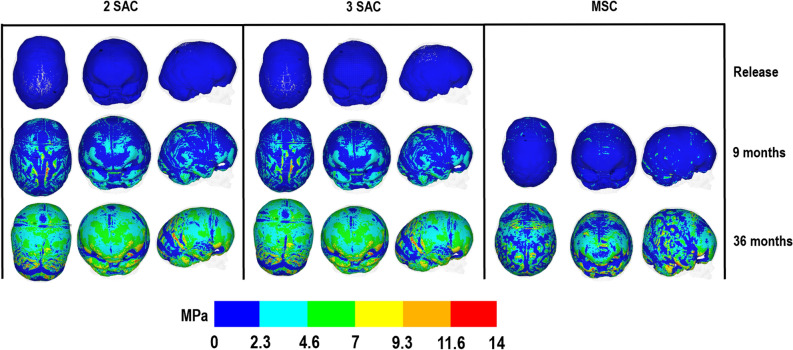
Sagittal synostosis is the most occurring form of craniosynostosis, resulting in calvarial deformation and possible long-term neurocognitive deficits. Several surgical techniques have been developed to correct these issues. Debates as to the most optimal approach are still ongoing. Finite element method is a computational tool that's shown to assist with the management of craniosynostosis. The aim of this study was to compare and predict the outcomes of three reconstruction methods for sagittal craniosynostosis. Here, a generic finite element model was developed based on a patient at 4 months of age and was virtually reconstructed under all three different techniques. Calvarial growth was simulated to predict the skull morphology and the impact of different reconstruction techniques on the brain growth up to 60 months of age. Predicted morphology was then compared with in vivo and literature data. Our results show a promising resemblance to morphological outcomes at follow up. Morphological characteristics between considered techniques were also captured in our predictions. Pressure outcomes across the brain highlight the potential impact that different techniques have on growth. This study lays the foundation for further investigation into additional reconstructive techniques for sagittal synostosis with the long-term vision of optimizing the management of craniosynostosis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
