

A Novel Cause of Bowel Obstruction in a Patient with Long-Standing Crohn's Disease
- PMID: 34707913
- PMCID: PMC8545553
- DOI: 10.1155/2021/3278392
A Novel Cause of Bowel Obstruction in a Patient with Long-Standing Crohn's Disease
Abstract
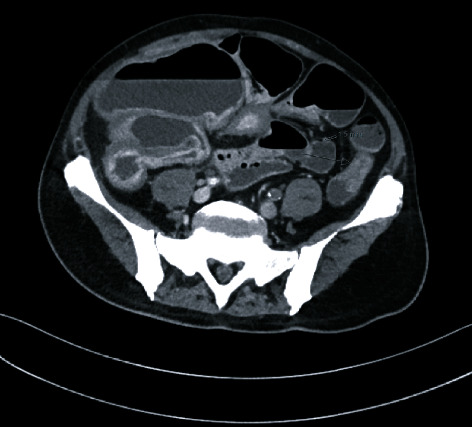
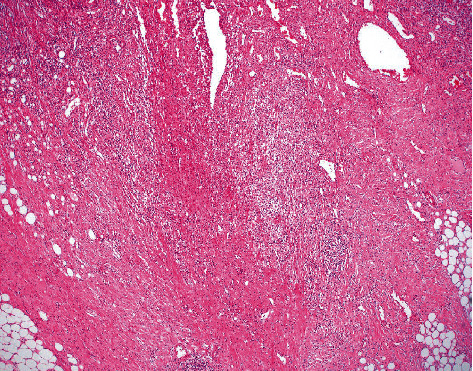
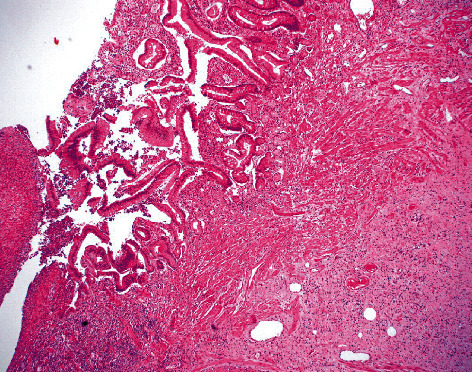
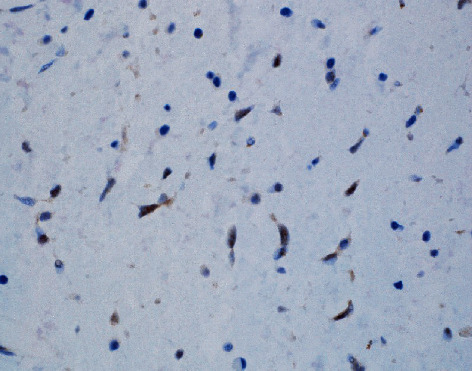
Solitary fibrous tumors are rare tumors of mesenchymal origin. Although most often observed in the lung pleura, they have been reported in varied extrapleural sites. A 70-year-old male with complicated Crohn's disease presented with 3 days of nausea, emesis, constipation, and abdominal pain. Computed Tomography (CT) demonstrated mucosal thickening of the middescending colon, consistent with fibrosing stricture. Surgical excision revealed an unusual, 5 cm mass originating in the subserosa. Histopathology of the lesion was notable for a proliferation of cells with spindle and stellate-shaped nuclei and no appreciable mitotic figures, which extended into the muscularis and submucosa. Immunohistochemistry was STAT6 nuclear positive and cytoplasmic CD34 positive, diagnostic for solitary fibrous tumor (SFT). In this case, the SFT infiltrating into the muscularis propria and subserosa caused the stricture and bowel obstruction. This illustrates that while fibrosing strictures are usually the etiology of bowel obstruction in the setting of Crohn's disease, other rare possible causes should be considered.
Copyright © 2021 Satya V. Vedula et al.
Conflict of interest statement
The authors have no conflict of interest to report.
Figures


Similar articles
-
Solitary fibrous tumor: A rare lesion with an unusual paravertebral presentation.Am J Otolaryngol. 2022 Sep-Oct;43(5):103588. doi: 10.1016/j.amjoto.2022.103588. Epub 2022 Aug 6. Am J Otolaryngol. 2022. PMID: 35953391
-
Extrapleural solitary fibrous tumor: A distinct entity from pleural solitary fibrous tumor. An update on clinical, molecular and diagnostic features.Ann Diagn Pathol. 2018 Jun;34:142-150. doi: 10.1016/j.anndiagpath.2018.01.004. Epub 2018 Apr 9. Ann Diagn Pathol. 2018. PMID: 29660566 Review.
-
Malignant Extrapleural Solitary Fibrous Tumor.Cureus. 2023 Aug 19;15(8):e43750. doi: 10.7759/cureus.43750. eCollection 2023 Aug. Cureus. 2023. PMID: 37605717 Free PMC article.
-
Phytobezoar causing small bowel obstruction in a patient with Crohn's disease: A case report.Int J Surg Case Rep. 2022 Oct;99:107615. doi: 10.1016/j.ijscr.2022.107615. Epub 2022 Sep 8. Int J Surg Case Rep. 2022. PMID: 36108380 Free PMC article.
-
An unusual location of solitary fibrous tumor in heart-A case report and review of literature.Cancer Rep (Hoboken). 2022 Nov;5(11):e1698. doi: 10.1002/cnr2.1698. Epub 2022 Aug 30. Cancer Rep (Hoboken). 2022. PMID: 36041816 Free PMC article. Review.
References
-
- Vythianathan M., Yong J. A rare primary malignant solitary fibrous tumour of the liver. Pathology . 2013;45:S86–S87. doi: 10.1097/01.PAT.0000426954.68370.26. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
