

S-GRAS score for prognostic classification of adrenocortical carcinoma: an international, multicenter ENSAT study
- PMID: 34709200
- PMCID: PMC8679848
- DOI: 10.1530/EJE-21-0510
S-GRAS score for prognostic classification of adrenocortical carcinoma: an international, multicenter ENSAT study
Abstract
Objective: Adrenocortical carcinoma (ACC) has an aggressive but variable clinical course. Prognostic stratification based on the European Network for the Study of Adrenal Tumours stage and Ki67 index is limited. We aimed to demonstrate the prognostic role of a points-based score (S-GRAS) in a large cohort of patients with ACC.
Design: This is a multicentre, retrospective study on ACC patients who underwent adrenalectomy.
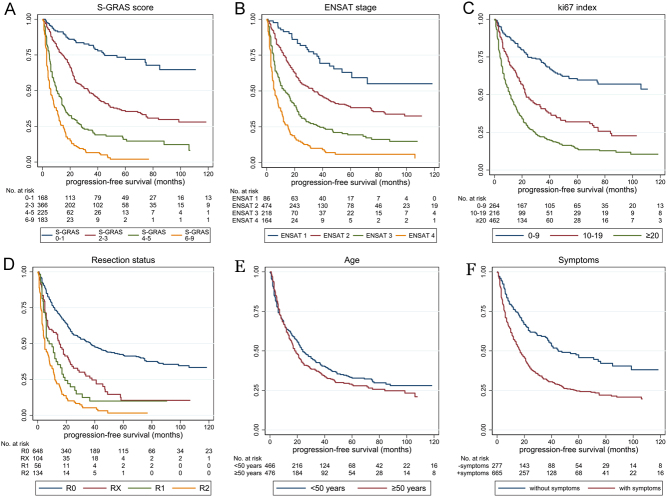
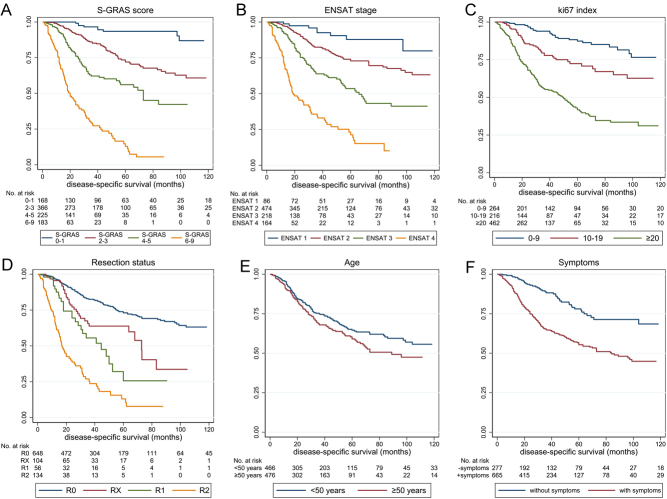
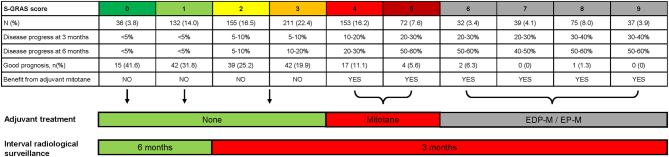
Methods: The S-GRAS score was calculated as a sum of the following points: tumour stage (1-2 = 0; 3 = 1; 4 = 2), grade (Ki67 index 0-9% = 0; 10-19% = 1; ≥20% = 2 points), resection status (R0 = 0; RX = 1; R1 = 2; R2 = 3), age (<50 years = 0; ≥50 years = 1), symptoms (no = 0; yes = 1), and categorised, generating four groups (0-1, 2-3, 4-5, and 6-9). Endpoints were progression-free survival (PFS) and disease-specific survival (DSS). The discriminative performance of S-GRAS and its components was tested by Harrell's Concordance index (C-index) and Royston-Sauerbrei's R2D statistic.
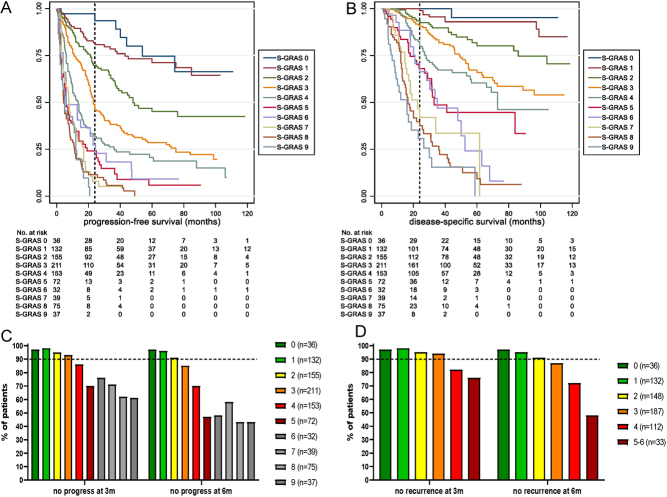
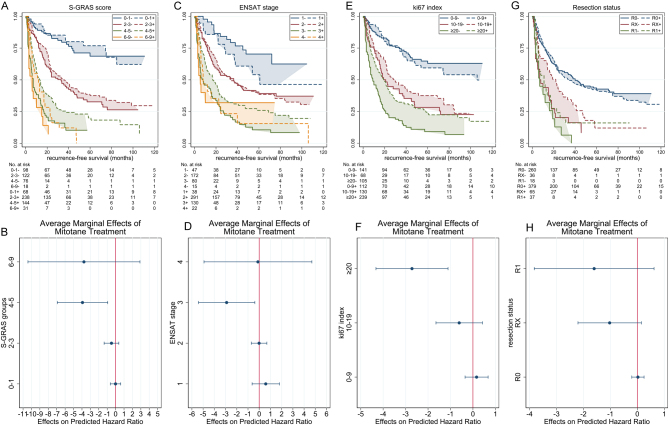
Results: We included 942 ACC patients. The S-GRAS score showed superior prognostic performance for both PFS and DSS, with best discrimination obtained using the individual scores (0-9) (C-index = 0.73, R2D = 0.30, and C-index = 0.79, R2D = 0.45, respectively, all P < 0.01vs each component). The superiority of S-GRAS score remained when comparing patients treated or not with adjuvant mitotane (n = 481 vs 314). In particular, the risk of recurrence was significantly reduced as a result of adjuvant mitotane only in patients with S-GRAS 4-5.
Conclusion: The prognostic performance of S-GRAS is superior to tumour stage and Ki67 in operated ACC patients, independently from adjuvant mitotane. S-GRAS score provides a new important guide for personalised management of ACC (i.e. radiological surveillance and adjuvant treatment).
Figures
References
-
- Kerkhofs TMA, Verhoeven RHA, Van Der Zwan JM, Dieleman J, Kerstens MN, Links TP, Van de Poll-Franse LV, Haak HR. Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. European Journal of Cancer 2013492579–2586. ( 10.1016/j.ejca.2013.02.034) - DOI - PubMed
-
- Fassnacht M, Johanssen S, Quinkler M, Bucsky P, Willenberg HS, Beuschlein F, Terzolo M, Mueller HH, Hahner S, Allolio Bet al. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a revised TNM classification. Cancer 2009115243–250. ( 10.1002/cncr.24030) - DOI - PubMed
-
- Else T, Williams AR, Sabolch A, Jolly S, Miller BS, Hammer GD. Adjuvant therapies and patient and tumor characteristics associated with survival of adult patients with adrenocortical carcinoma. Journal of Clinical Endocrinology and Metabolism 201499455–461. ( 10.1210/jc.2013-2856) - DOI - PMC - PubMed
-
- Calabrese A, Basile V, Puglisi S, Perotti P, Pia A, Saba L, Berchialla P, Porpiglia F, Veltri A, Volante Met al. Adjuvant mitotane therapy is beneficial in non-metastatic adrenocortical carcinoma at high risk of recurrence. European Journal of Endocrinology 2019180387–396. ( 10.1530/EJE-18-0923) - DOI - PubMed
