

doi: 10.36660/abc.20210788.
Update of the Brazilian Guideline for Familial Hypercholesterolemia - 2021
[Article in
English,
Portuguese]
Affiliations
- PMID: 34709306
- PMCID: PMC8528358
- DOI: 10.36660/abc.20210788
Item in Clipboard
Update of the Brazilian Guideline for Familial Hypercholesterolemia - 2021
[Article in
English,
Portuguese]
Arq Bras Cardiol.
2021 Oct.
No abstract available
Figures


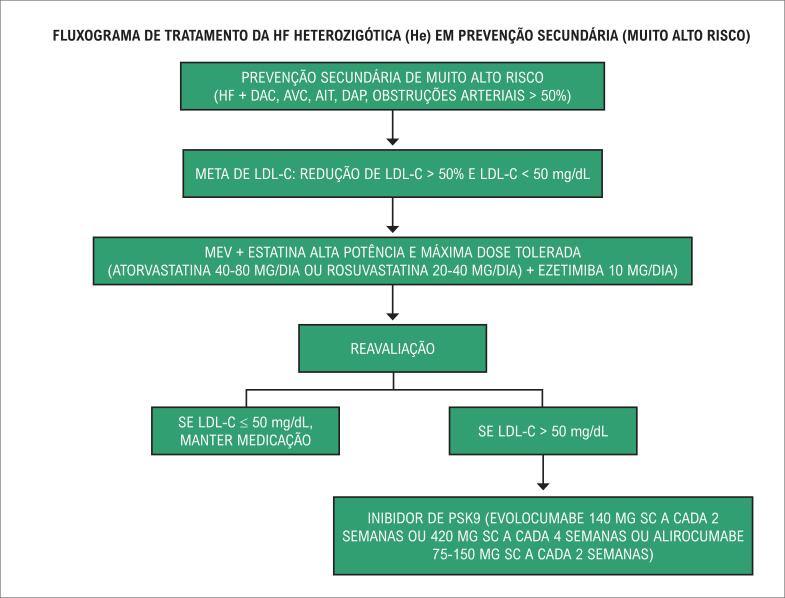
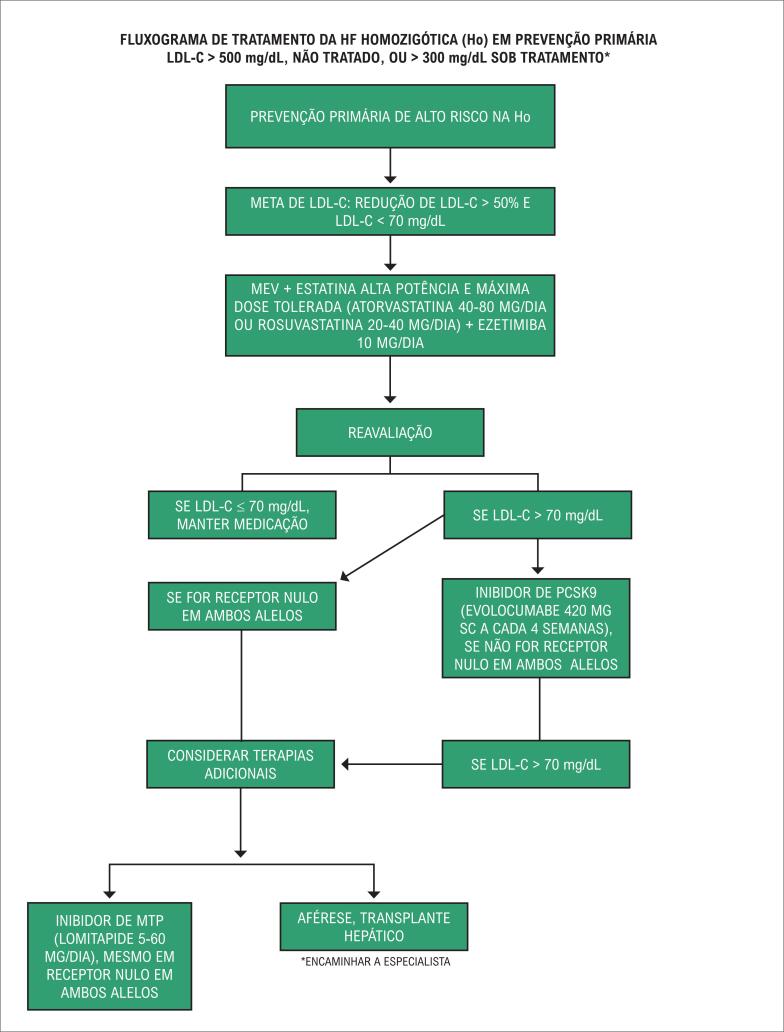
AIT: ataque isquêmico transitório; AVC: acidente vascular cerebral; DAC: doença arterial coronariana; DAP: doença arterial periférica; HF: hipercolesterolemia familiar; LDL-C: colesterol da lipoproteína de baixa densidade; MEV: mudança de estilo de vida.
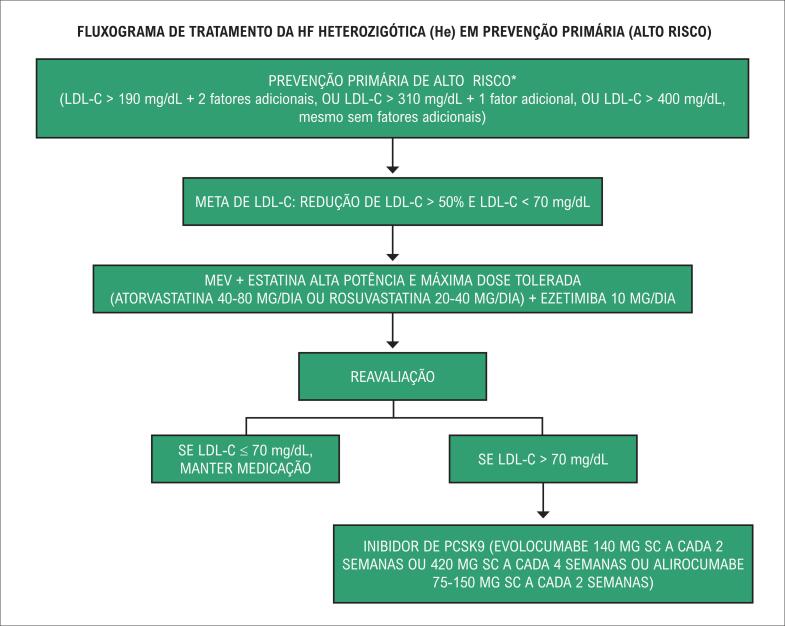
*São considerados fatores de risco adicionais na HF: idade > 40 anos e sem tratamento, tabagismo, sexo masculino, Lp(a) > 50 mg/dL, HDL-c < 40 mg/ dL, hipertensão arterial, diabetes melito, história familiar de DAC prematura em parentes de 1º grau (homens < 55 anos e mulheres < 60 anos), doença renal crônica (TFG < 60 ml/min) e IMC > 30 kg/m2.
*São considerados fatores de risco adicionais na HF: idade > 40 anos e sem tratamento, tabagismo, sexo masculino, Lp(a) > 50 mg/dL, HDL-c < 40 mg/ dL, hipertensão arterial, diabetes melito, história familiar de DAC prematura em parentes de 1º grau (homens < 55 anos e mulheres < 60 anos), doença renal crônica (TFG < 60 ml/min) e IMC > 30 kg/m2.
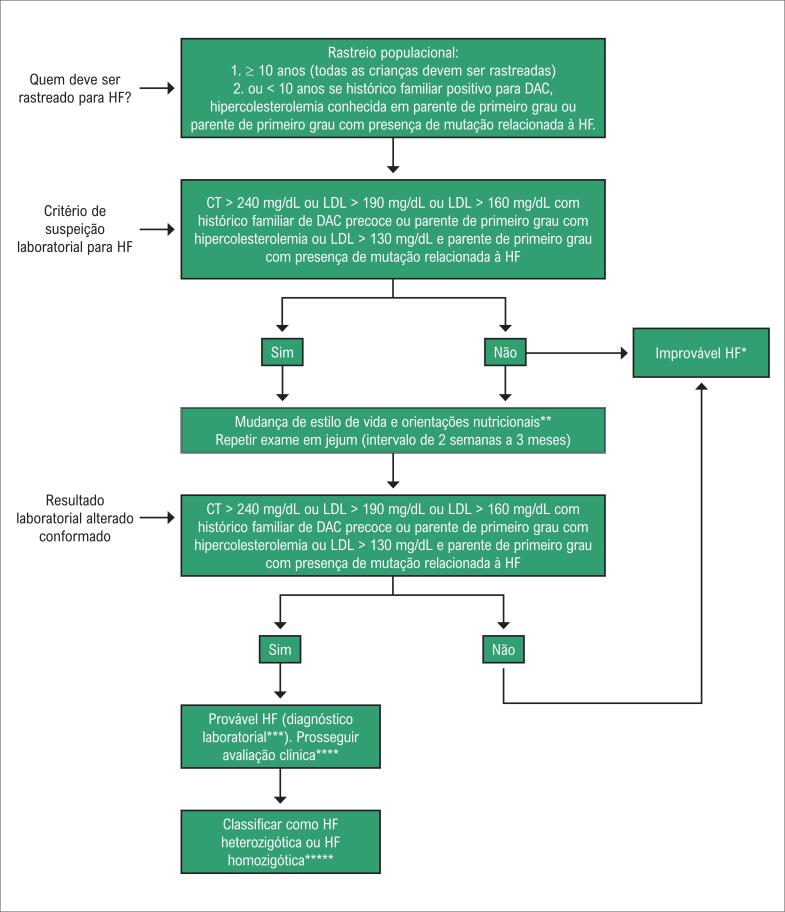
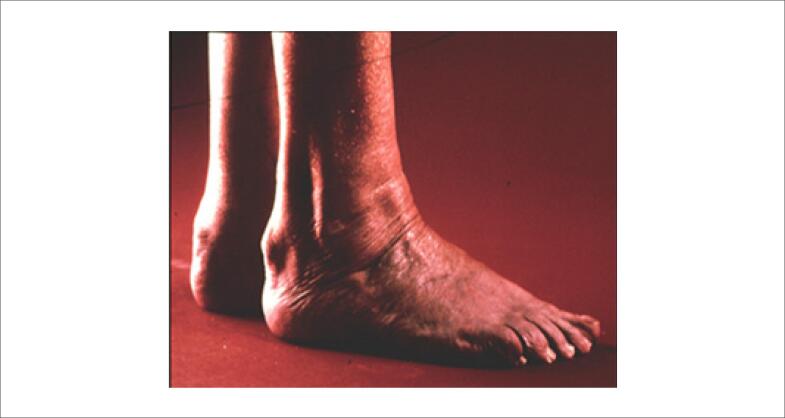
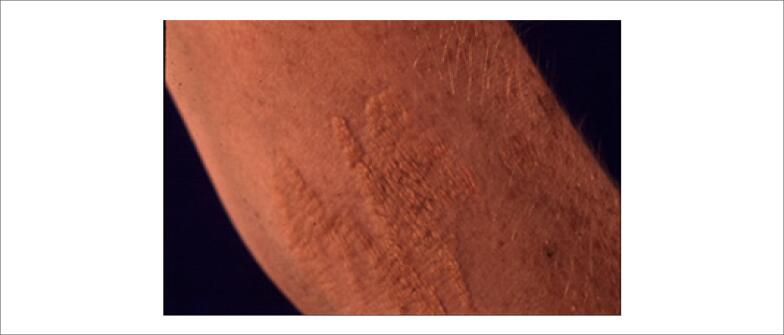
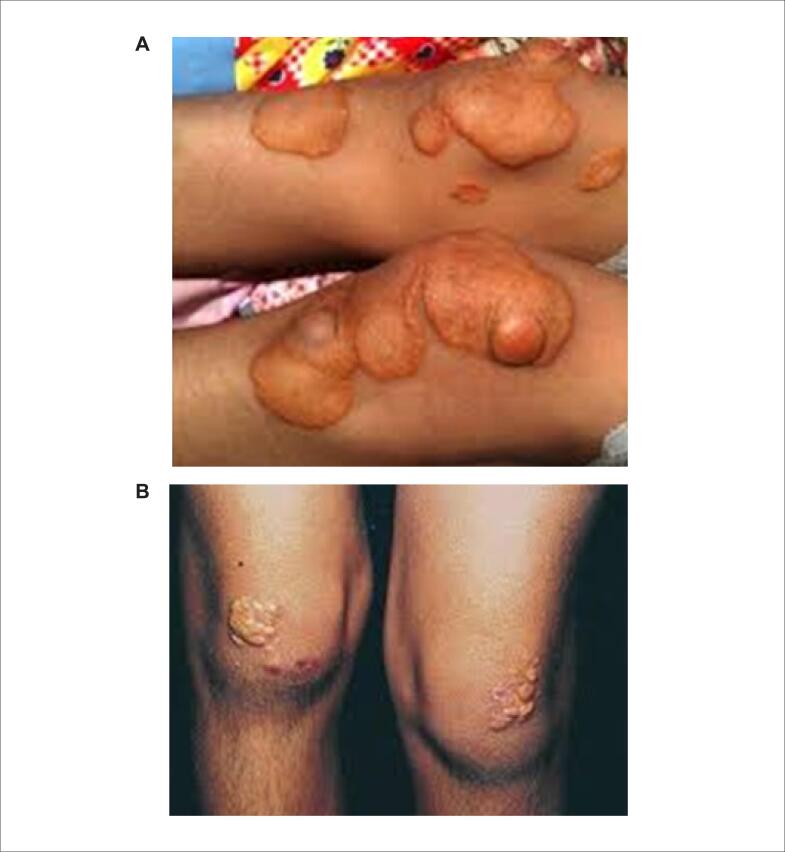
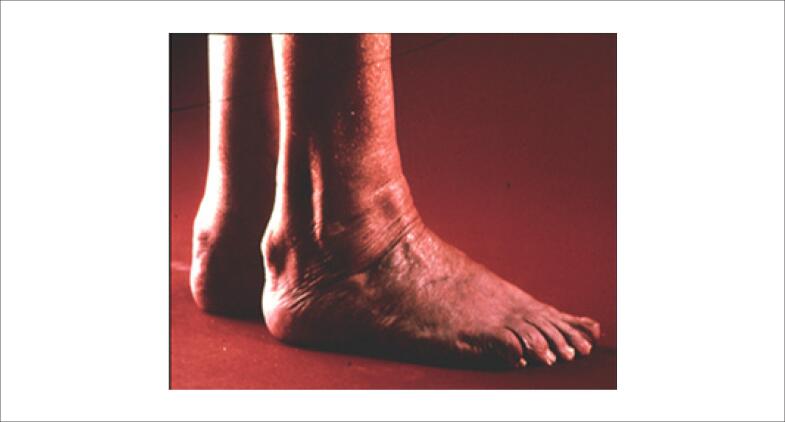
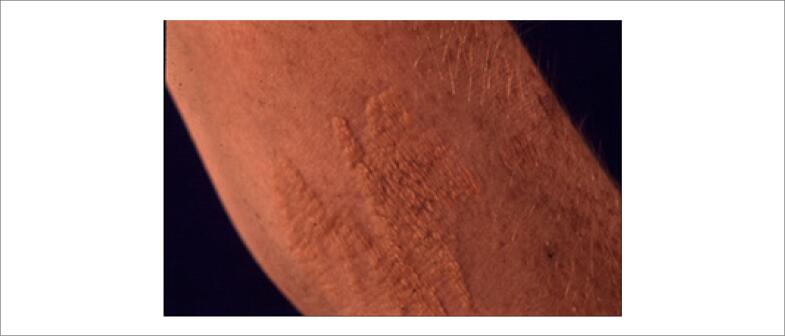
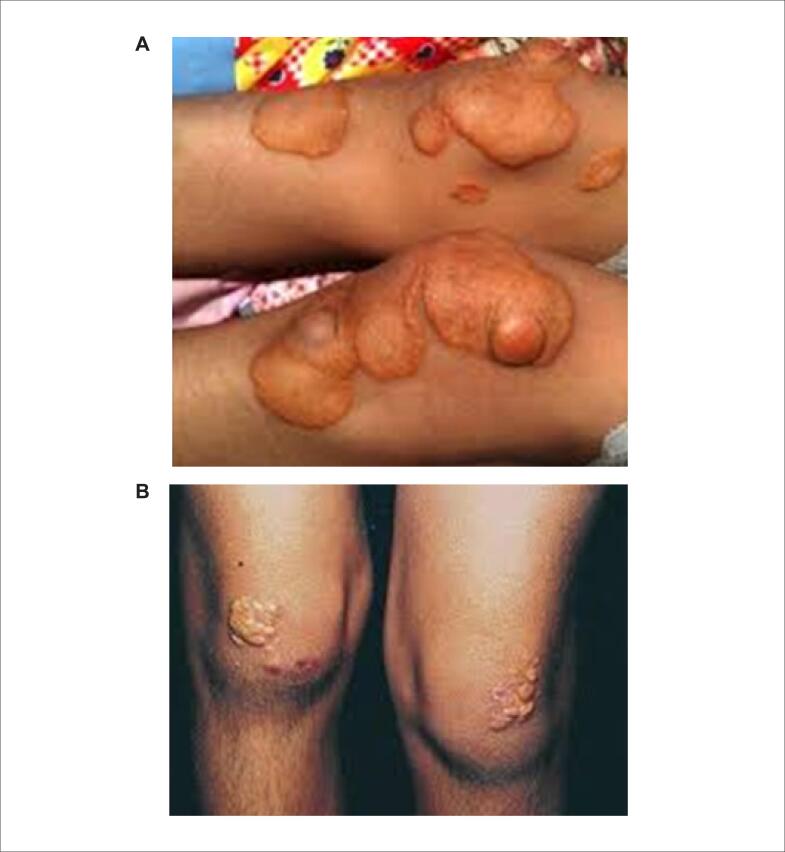
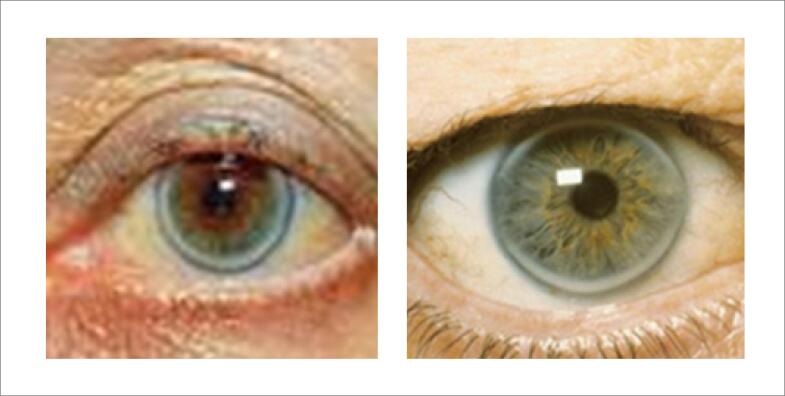
DAC: Doença arterial coronariana; HF: hipercolesterolemia familiar; CT: Colesterol total; LDL: Low-density lipoprotein. *Improvável HF: a ausência de critérios laboratoriais para HF não significa que outra dislipidemia não esteja presente. A criança ou adolescente com níveis de perfil lipídico fora do valor de referência para sua faixa etária deverá seguir com avaliação clínica. Importante avaliar causas secundárias nesta faixa etária: disfunção renal, tireoidiana, HIV, doenças auto-imunes, diabetes e obesidade, dentre outras. **Mudança de estilo de vida e orientação nutricional; vide seção terapia não farmacológica. ***Quando disponível o teste genético deve ser ofertado. ****Avaliação clínica: sinais clínicos como xantomas, xantelasma, arco corneano e espessamento de tendões devem ser avaliados. Descartar condições clínicas não HF que cursam com hipercolesterolemia. Escores de Dutch devem ser aplicados nesta etapa. *****Vide seção: Particularidades no manejo do paciente com HFo
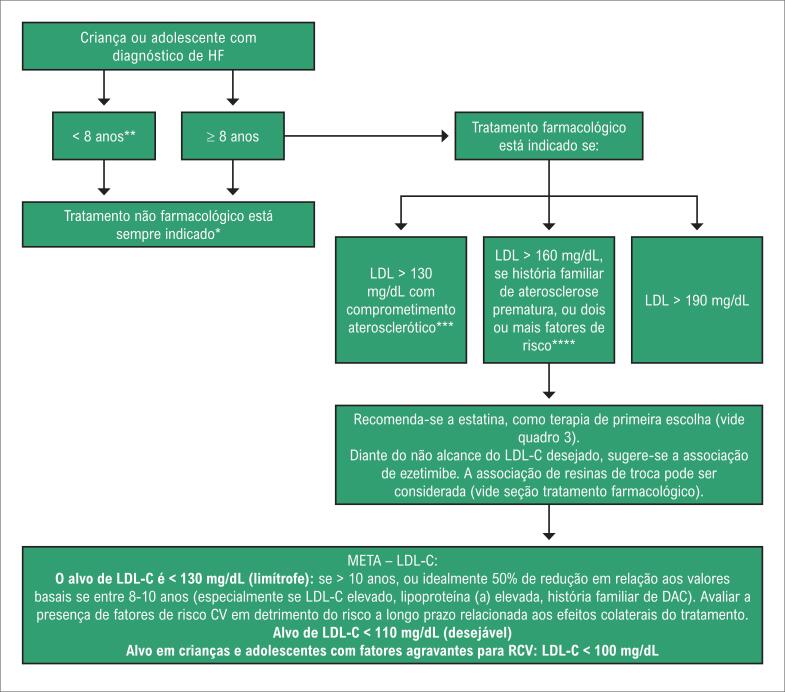
HF: hipercolesterolemia familiar; LDL: Low-density lipoprotein; DAC: Doença Arterial Coronariana; RCV: Risco Cardiovascular. *Todas as crianças devem ser submetidas a terapia não farmacológica: Vide seção terapia não farmacológica. **Em crianças menores de 8 anos a decisão por terapia farmacológica deverá ser avaliada de forma individualizada, em geral, para pacientes heterozigotos graves ou homozigotos. ***Se LDL > 130 mg/dL, sem comprometimento aterosclerótico, optar por tratamento não-farmacológico. ****Vide seção fatores relacionados ao aumento do RCV.

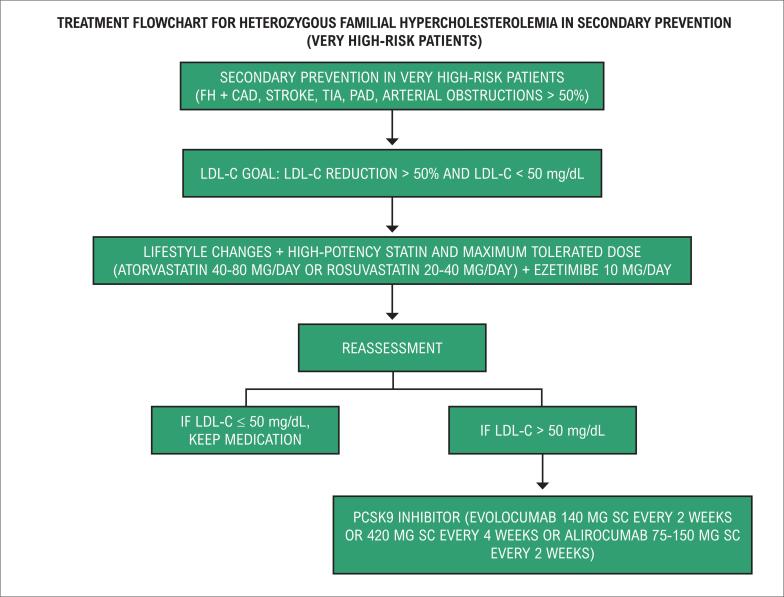
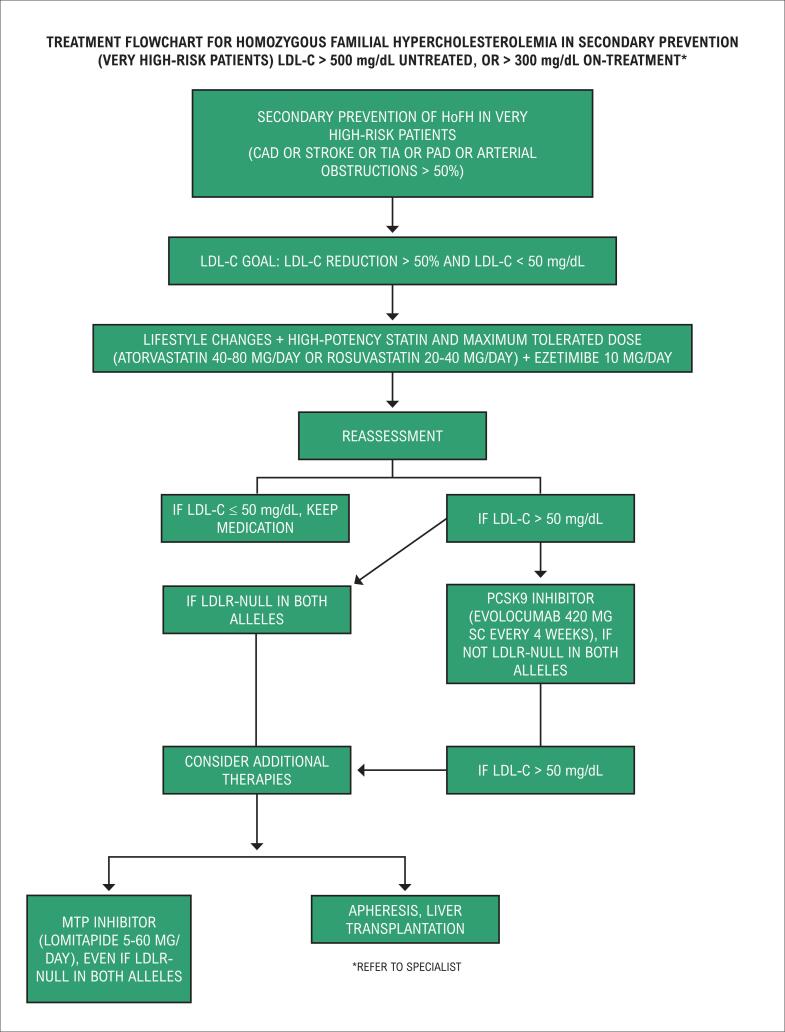
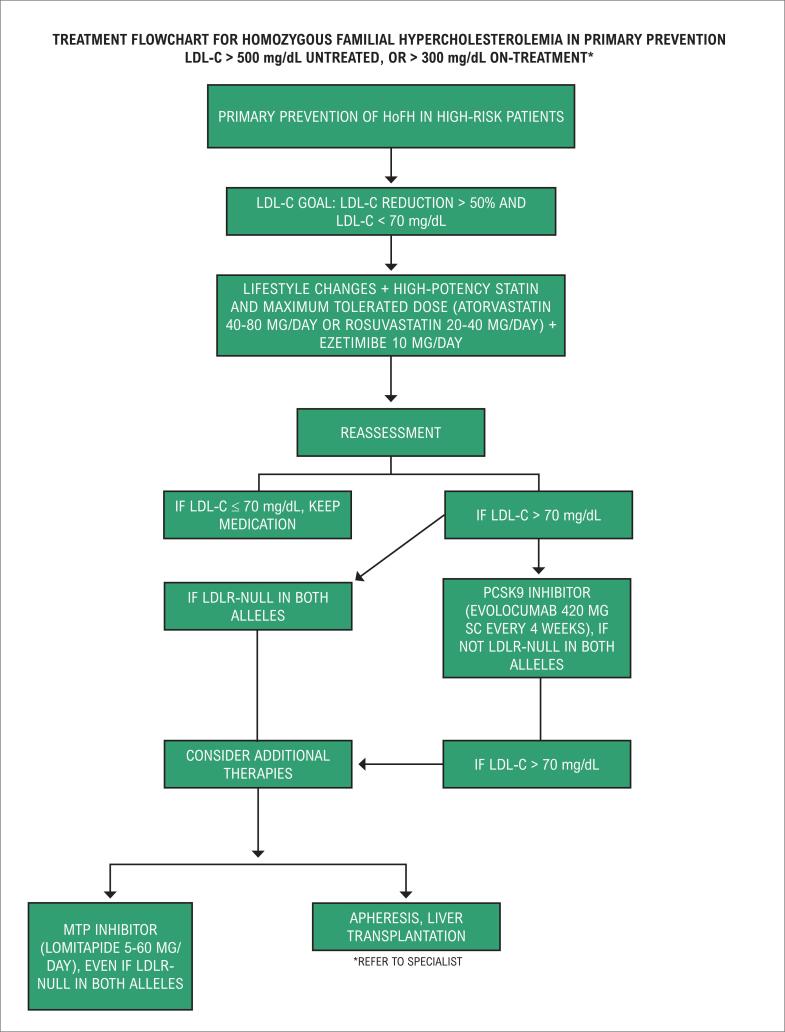
CAD: coronary artery disease; FH: familial hypercholesterolemia; LDL-C: low-density lipoprotein cholesterol; PAD: peripheral artery disease; SC: subcutaneously; TIA: transient ischemic attack.
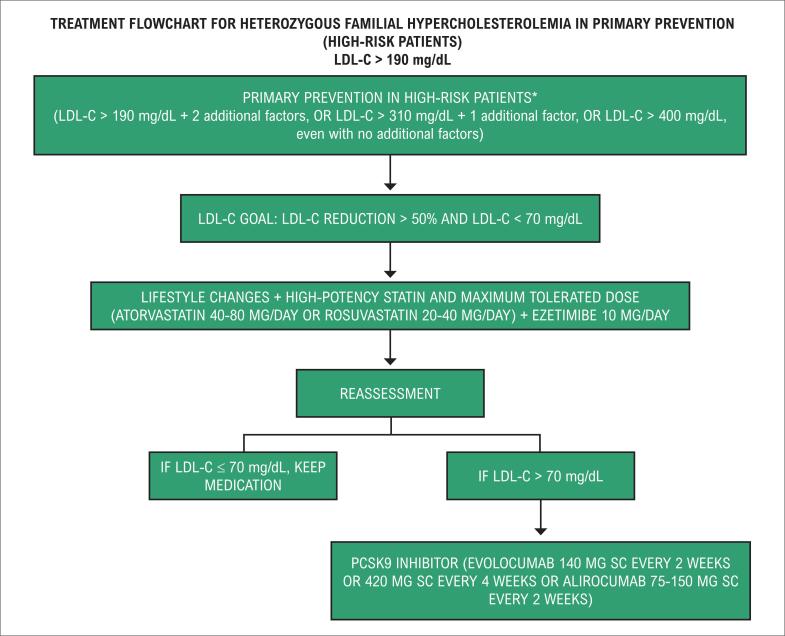
*Additional risk factors in FH are the following: age > 40 years and no treatment, smoking, being male, Lp(a) > 50 mg/dL, HDL-C < 40 mg/dL, hypertension, diabetes mellitus, family history of premature CAD in rst-degree relatives (men aged < 55 years and women aged < 60 years), chronic kidney disease (GFR < 60 mL/min), and BMI > 30 kg/m2.
*Additional risk factors in FH are the following: age > 40 years and no treatment, smoking, being male, Lp(a) > 50 mg/dL, HDL-C < 40 mg/dL, hypertension, diabetes mellitus, family history of premature CAD in rst-degree relatives (men aged < 55 years and women aged < 60 years), chronic kidney disease (GFR < 60 mL/min), and BMI > 30 kg/m2.
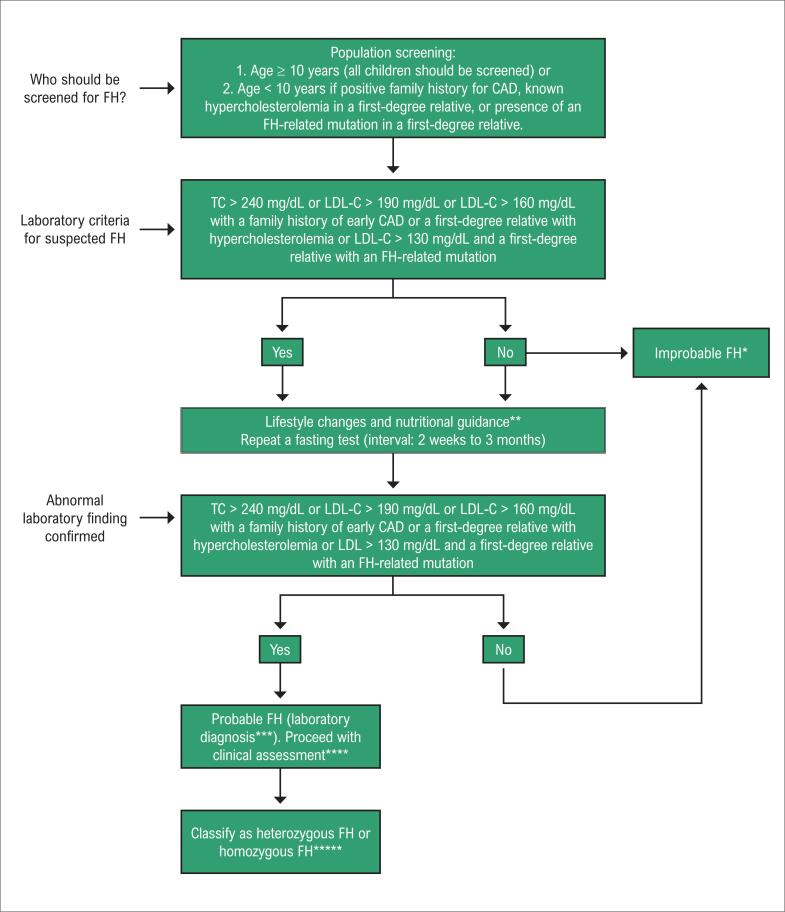
CAD: coronary artery disease; FH: familial hypercholesterolemia; LDL-C: low-density lipoprotein cholesterol; TC: total cholesterol. *Improbable FH: absence of laboratory criteria for FH does not mean that a different dyslipidemia is not present. Children or adolescents with lipid profile levels outside the reference range for their age group should undergo a clinical assessment. Secondary causes should be assessed in this age group: kidney or thyroid dysfunction, HIV, autoimmune diseases, diabetes, and obesity, among others. **Lifestyle changes and nutritional guidance; see nonpharmacological therapy section. ***When available, genetic testing should be provided. ****Clinical assessment: clinical signs such as xanthomas, xanthelasma, corneal arcus, and thickened tendon should be assessed. Rule out non-FH clinical conditions that co-occur with hypercholesterolemia. Dutch scores should be used at this stage. *****See peculiarities in the management of patients with HoFH section
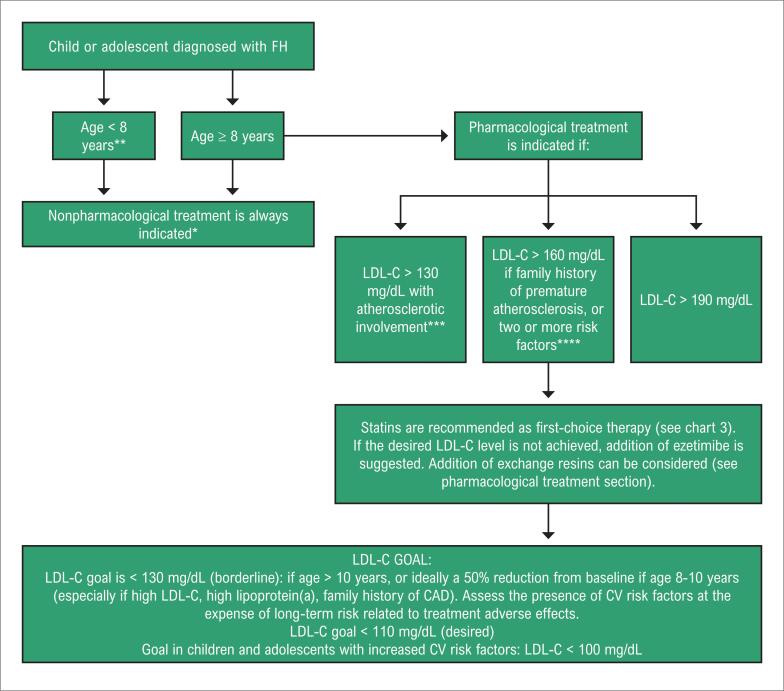
CAD: coronary artery disease; CV: cardiovascular; FH: familial hypercholesterolemia; LDL-C: low-density lipoprotein cholesterol. *All children should undergo a nonpharmacological therapy. See nonpharmacological therapy section. **In children under 8 years of age, the decision on drug therapy should be individualized, e.g. for cases of severe heterozygous or homozygous FH. ***If LDL-C > 130 mg/dL with no atherosclerotic involvement, choose nonpharmacological treatment. ****See factors related to increased cardiovascular risk section.
References
-
- Burns FS. A contribution to the study of the etiology of xanthoma multiplex. Arch Derm Syphilol. 1920;2(4):415–429.
- Burns FS. A contribution to the study of the etiology of xanthoma multiplex. Arch Derm Syphilol. 1920; 2(4):415-29.
-
- Müller C. Xanthomata, hypercholesterolemia and angina pectoris. Acta Med Scand Suppl. 1938;89:75–84.
- Müller C. Xanthomata, hypercholesterolemia and angina pectoris. Acta Med Scand Suppl. 1938; 89:75-84.
-
- Brown MS, Goldstein JL. Analysis of a mutant strain of human fibroblasts with a defect in the internalization of receptor bound low density lipoprotein. Cell. 1976;9(4 Pt 2):663–674. - PubMed
- Brown MS, Goldstein JL. Analysis of a mutant strain of human fibroblasts with a defect in the internalization of receptor bound low density lipoprotein. Cell. 1976; 9(4 Pt 2):663-74. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
