

Tissue Proteomic Analysis Identifies Mechanisms and Stages of Immunopathology in Fatal COVID-19
- PMID: 34710339
- PMCID: PMC8845132
- DOI: 10.1165/rcmb.2021-0358OC
Tissue Proteomic Analysis Identifies Mechanisms and Stages of Immunopathology in Fatal COVID-19
Abstract
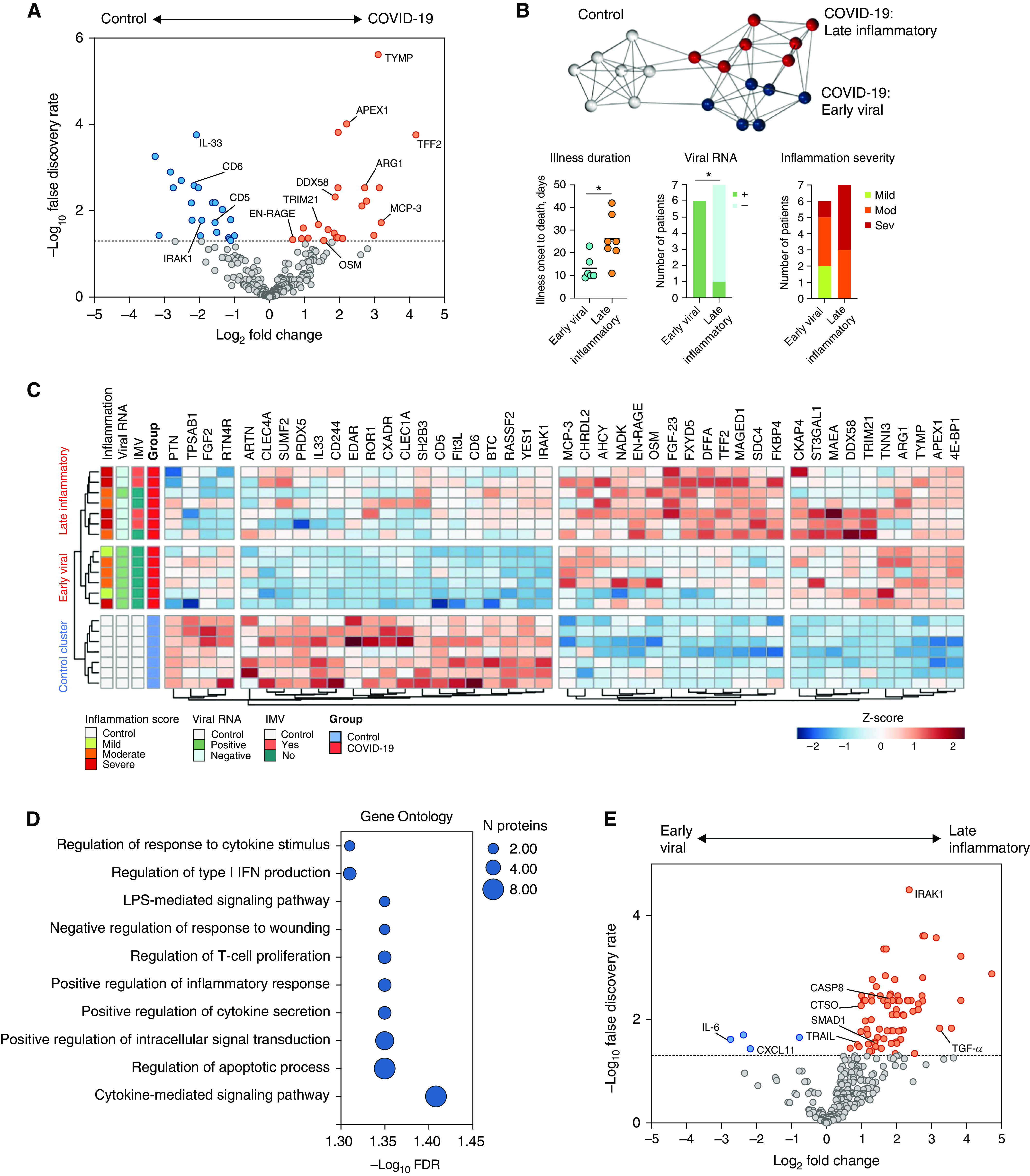
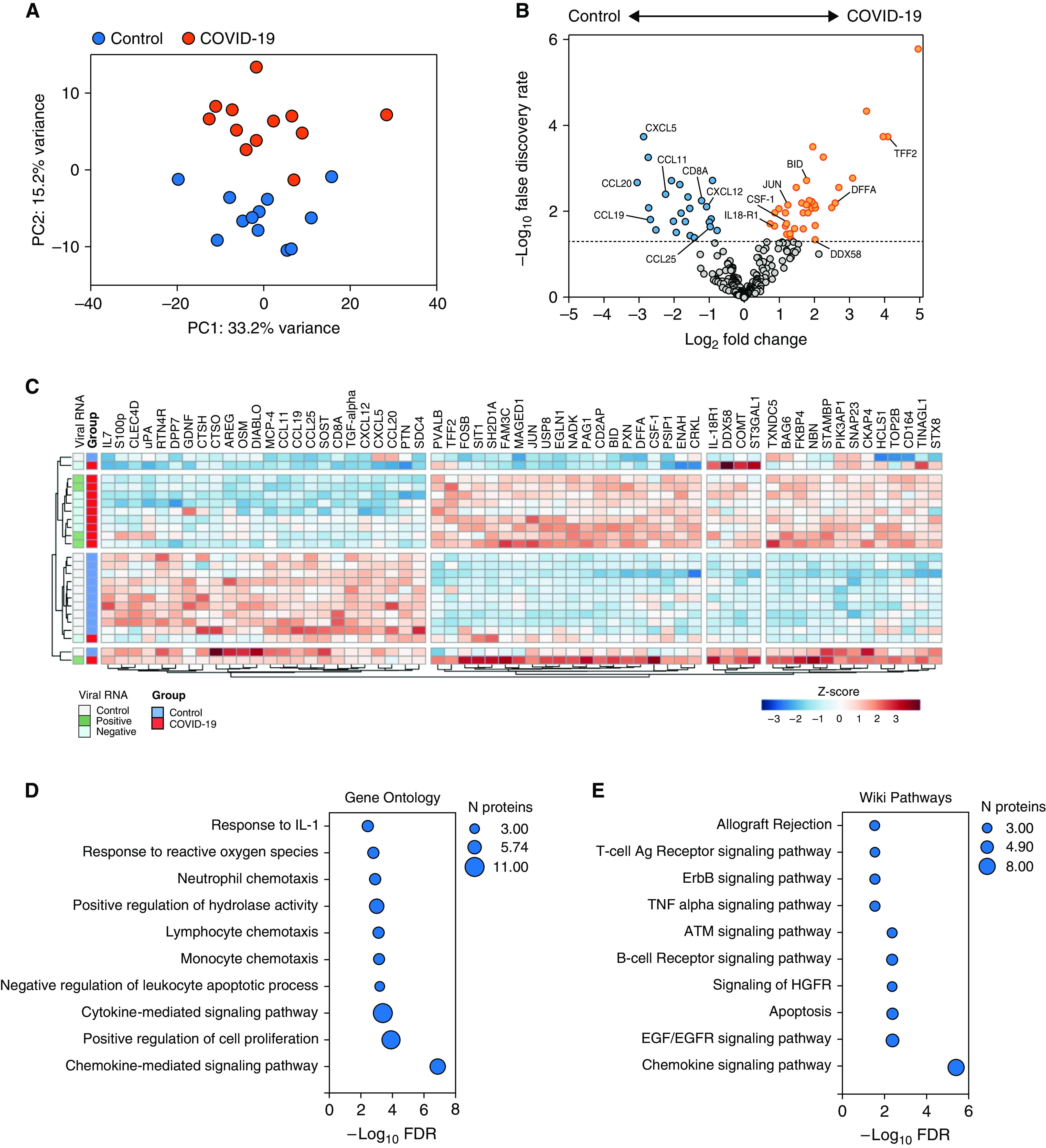
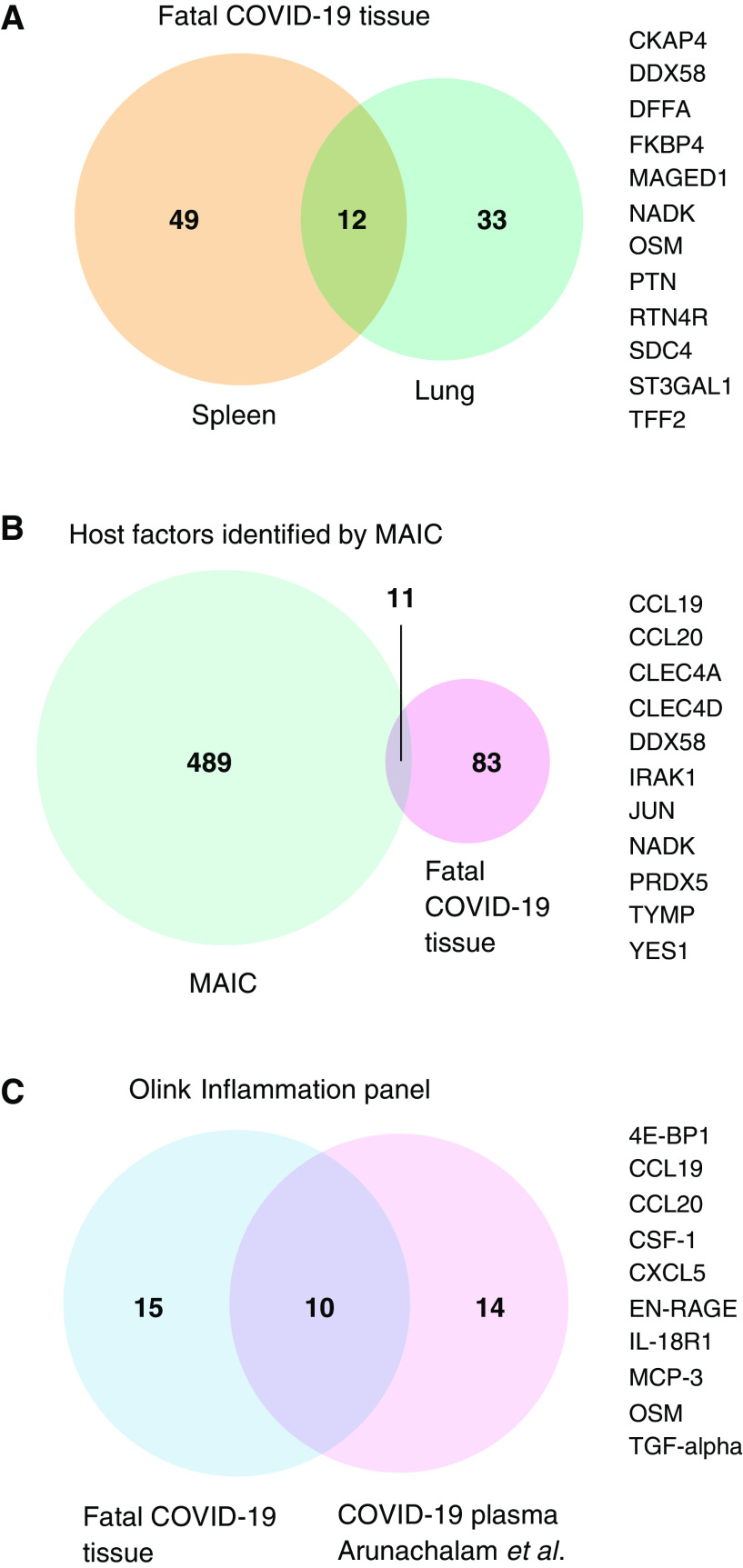
Immunopathology occurs in the lung and spleen in fatal coronavirus disease (COVID-19), involving monocytes/macrophages and plasma cells. Antiinflammatory therapy reduces mortality, but additional therapeutic targets are required. We aimed to gain mechanistic insight into COVID-19 immunopathology by targeted proteomic analysis of pulmonary and splenic tissues. Lung parenchymal and splenic tissue was obtained from 13 postmortem examinations of patients with fatal COVID-19. Control tissue was obtained from cancer resection samples (lung) and deceased organ donors (spleen). Protein was extracted from tissue by phenol extraction. Olink multiplex immunoassay panels were used for protein detection and quantification. Proteins with increased abundance in the lung included MCP-3, antiviral TRIM21, and prothrombotic TYMP. OSM and EN-RAGE/S100A12 abundance was correlated and associated with inflammation severity. Unsupervised clustering identified "early viral" and "late inflammatory" clusters with distinct protein abundance profiles, and differences in illness duration before death and presence of viral RNA. In the spleen, lymphocyte chemotactic factors and CD8A were decreased in abundance, and proapoptotic factors were increased. B-cell receptor signaling pathway components and macrophage colony stimulating factor (CSF-1) were also increased. Additional evidence for a subset of host factors (including DDX58, OSM, TYMP, IL-18, MCP-3, and CSF-1) was provided by overlap between 1) differential abundance in spleen and lung tissue; 2) meta-analysis of existing datasets; and 3) plasma proteomic data. This proteomic analysis of lung parenchymal and splenic tissue from fatal COVID-19 provides mechanistic insight into tissue antiviral responses, inflammation and disease stages, macrophage involvement, pulmonary thrombosis, splenic B-cell activation, and lymphocyte depletion.
Keywords: COVID-19; inflammation; lung; macrophages; proteomics.
Figures
Comment in
-
Understanding COVID-19 Pathophysiology: What Defines Progress?Am J Respir Cell Mol Biol. 2022 Feb;66(2):120-121. doi: 10.1165/rcmb.2021-0452ED. Am J Respir Cell Mol Biol. 2022. PMID: 34758278 Free PMC article. No abstract available.
References
-
- Menter T, Haslbauer JD, Nienhold R, Savic S, Hopfer H, Deigendesch N, et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology . 2020;77:198–209. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
