

Adaptive proton therapy
- PMID: 34710858
- PMCID: PMC8628198
- DOI: 10.1088/1361-6560/ac344f
Adaptive proton therapy
Abstract
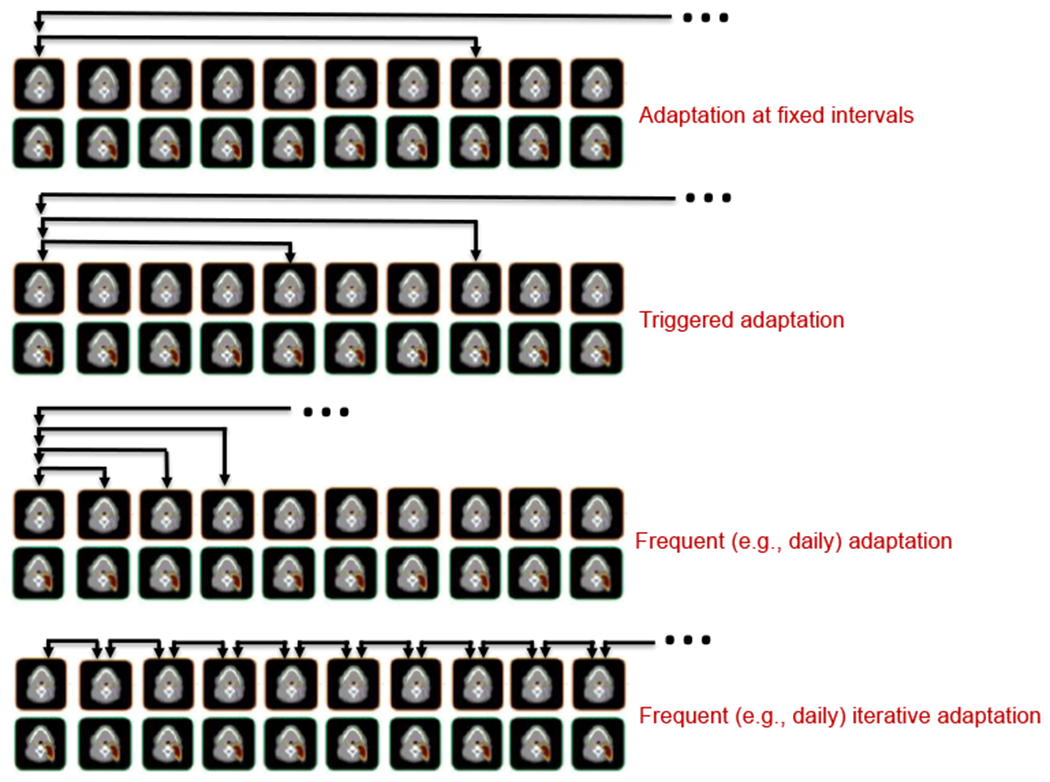
Radiation therapy treatments are typically planned based on a single image set, assuming that the patient's anatomy and its position relative to the delivery system remains constant during the course of treatment. Similarly, the prescription dose assumes constant biological dose-response over the treatment course. However, variations can and do occur on multiple time scales. For treatment sites with significant intra-fractional motion, geometric changes happen over seconds or minutes, while biological considerations change over days or weeks. At an intermediate timescale, geometric changes occur between daily treatment fractions. Adaptive radiation therapy is applied to consider changes in patient anatomy during the course of fractionated treatment delivery. While traditionally adaptation has been done off-line with replanning based on new CT images, online treatment adaptation based on on-board imaging has gained momentum in recent years due to advanced imaging techniques combined with treatment delivery systems. Adaptation is particularly important in proton therapy where small changes in patient anatomy can lead to significant dose perturbations due to the dose conformality and finite range of proton beams. This review summarizes the current state-of-the-art of on-line adaptive proton therapy and identifies areas requiring further research.
Keywords: adaptive radiation therapy; online adaptation; proton therapy.
© 2021 Institute of Physics and Engineering in Medicine.
Figures

References
-
- Ahunbay EE, Peng C, Chen GP, Narayanan S, Yu C, Lawton C and Li XA 2008. An on-line replanning scheme for interfractional variations Med Phys 35 3607–15 - PubMed
-
- Amstutz F, Nenoff L, Albertini F, Ribeiro CO, Knopf AC, Unkelbach J, Weber DC, Lomax AJ and Zhang Y 2021. An approach for estimating dosimetric uncertainties in deformable dose accumulation in pencil beam scanning proton therapy for lung cancer Phys Med Biol 66 - PubMed
-
- Arai K, Kadoya N, Kato T, Endo H, Komori S, Abe Y, Nakamura T, Wada H, Kikuchi Y, Takai Y and Jingu K 2017. Feasibility of CBCT-based proton dose calculation using a histogram-matching algorithm in proton beam therapy Phys Med 33 68–76 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
