

Novel temporal and spatial patterns of metastatic colonization from breast cancer rapid-autopsy tumor biopsies
- PMID: 34711268
- PMCID: PMC8555066
- DOI: 10.1186/s13073-021-00989-6
Novel temporal and spatial patterns of metastatic colonization from breast cancer rapid-autopsy tumor biopsies
Abstract
Background: Metastatic breast cancer is a deadly disease with a low 5-year survival rate. Tracking metastatic spread in living patients is difficult and thus poorly understood.
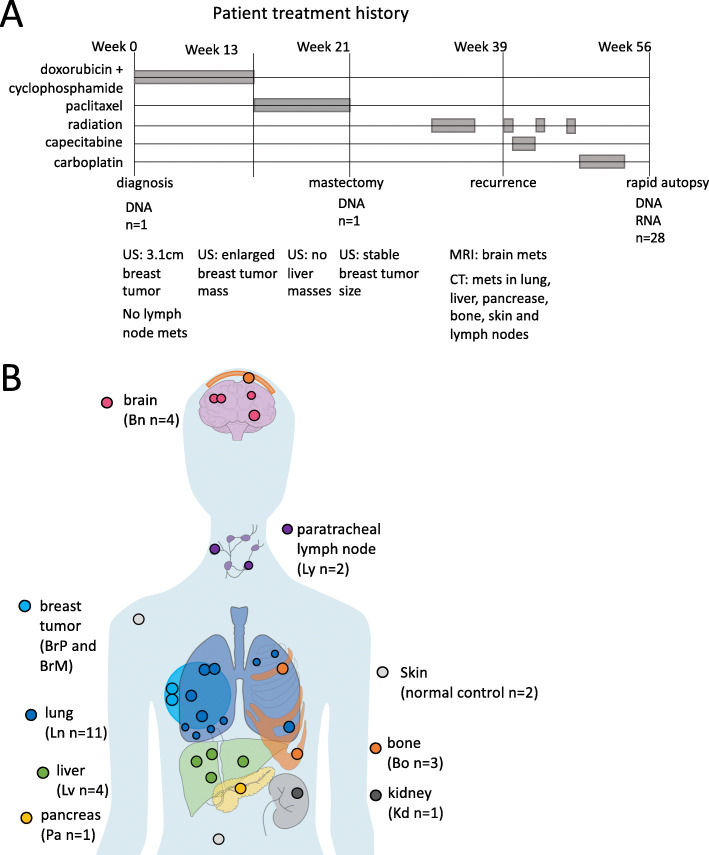
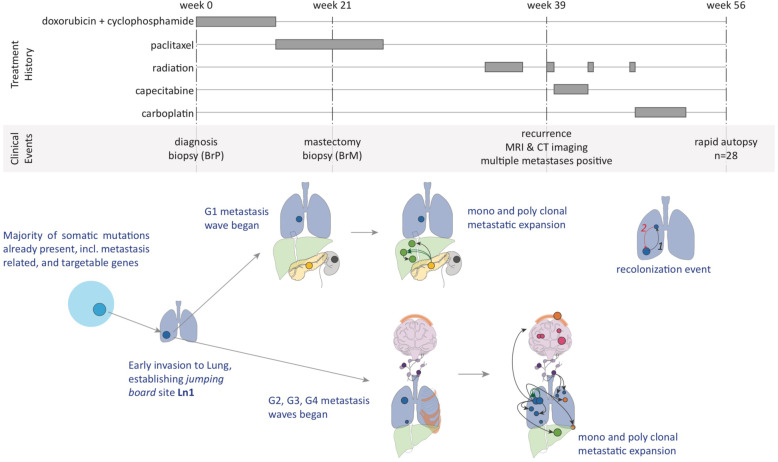
Methods: Via rapid autopsy, we have collected 30 tumor samples over 3 timepoints and across 8 organs from a triple-negative metastatic breast cancer patient. The large number of sites sampled, together with deep whole-genome sequencing and advanced computational analysis, allowed us to comprehensively reconstruct the tumor's evolution at subclonal resolution.
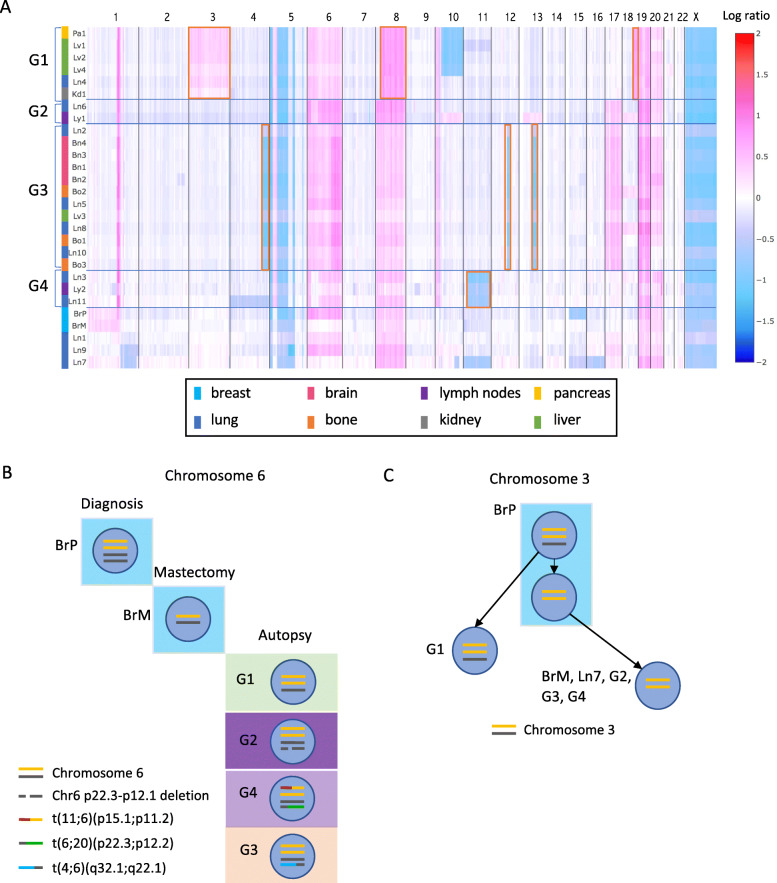
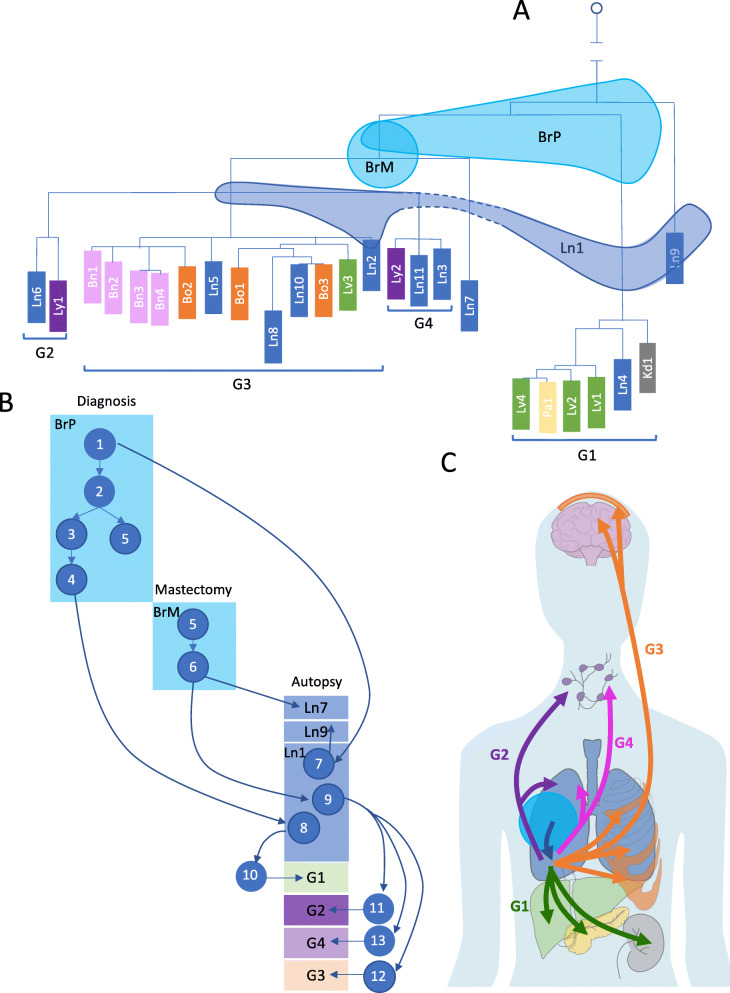
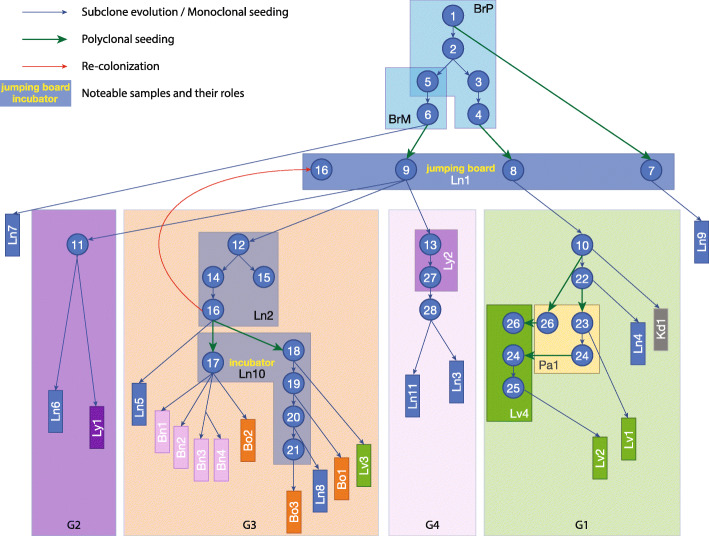
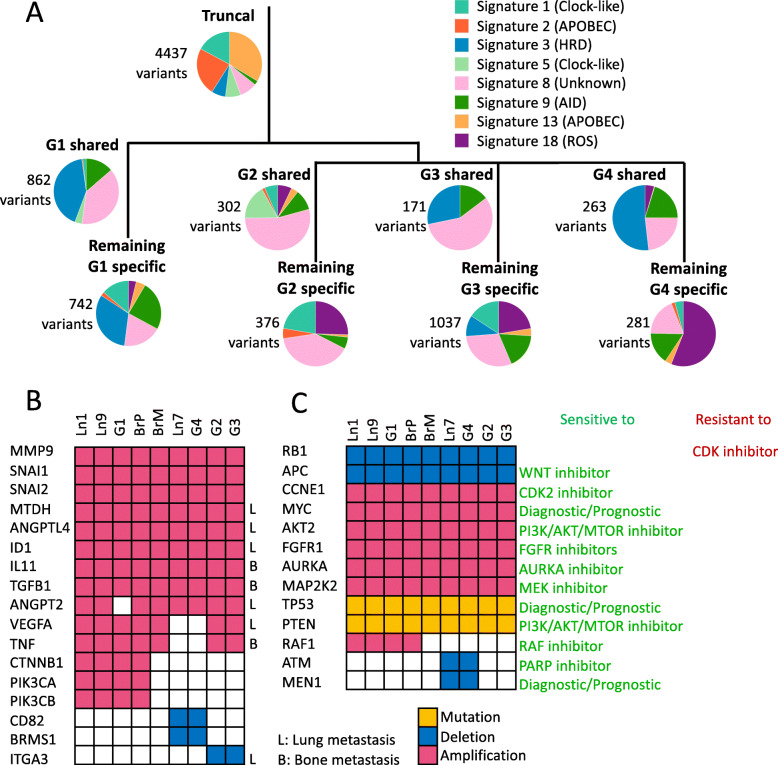
Results: The most unique, previously unreported aspect of the tumor's evolution that we observed in this patient was the presence of "subclone incubators," defined as metastatic sites where substantial tumor evolution occurs before colonization of additional sites and organs by subclones that initially evolved at the incubator site. Overall, we identified four discrete waves of metastatic expansions, each of which resulted in a number of new, genetically similar metastasis sites that also enriched for particular organs (e.g., abdominal vs bone and brain). The lung played a critical role in facilitating metastatic spread in this patient: the lung was the first site of metastatic escape from the primary breast lesion, subclones at this site were likely the source of all four subsequent metastatic waves, and multiple sites in the lung acted as subclone incubators. Finally, functional annotation revealed that many known drivers or metastasis-promoting tumor mutations in this patient were shared by some, but not all metastatic sites, highlighting the need for more comprehensive surveys of a patient's metastases for effective clinical intervention.
Conclusions: Our analysis revealed the presence of substantial tumor evolution at metastatic incubator sites in a patient, with potentially important clinical implications. Our study demonstrated that sampling of a large number of metastatic sites affords unprecedented detail for studying metastatic evolution.
Keywords: Metastatic breast cancer; Subclone; Tumor evolution.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Banerji S, Cibulskis K, Rangel-Escareno C, Brown KK, Carter SL, Frederick AM, Lawrence MS, Sivachenko AY, Sougnez C, Zou L, Cortes ML, Fernandez-Lopez JC, Peng S, Ardlie KG, Auclair D, Bautista-Piña V, Duke F, Francis J, Jung J, Maffuz-Aziz A, Onofrio RC, Parkin M, Pho NH, Quintanar-Jurado V, Ramos AH, Rebollar-Vega R, Rodriguez-Cuevas S, Romero-Cordoba SL, Schumacher SE, Stransky N, Thompson KM, Uribe-Figueroa L, Baselga J, Beroukhim R, Polyak K, Sgroi DC, Richardson AL, Jimenez-Sanchez G, Lander ES, Gabriel SB, Garraway LA, Golub TR, Melendez-Zajgla J, Toker A, Getz G, Hidalgo-Miranda A, Meyerson M. Sequence analysis of mutations and translocations across breast cancer subtypes. Nature. 2012;486(7403):405–409. doi: 10.1038/nature11154. - DOI - PMC - PubMed
-
- Ciriello G, Gatza ML, Beck AH, Wilkerson MD, Rhie SK, Pastore A, Zhang H, McLellan M, Yau C, Kandoth C, Bowlby R, Shen H, Hayat S, Fieldhouse R, Lester SC, Tse GMK, Factor RE, Collins LC, Allison KH, Chen YY, Jensen K, Johnson NB, Oesterreich S, Mills GB, Cherniack AD, Robertson G, Benz C, Sander C, Laird PW, Hoadley KA, King TA, Perou CM, Akbani R, Auman JT, Balasundaram M, Balu S, Barr T, Beck A, Benz C, Benz S, Berrios M, Beroukhim R, Bodenheimer T, Boice L, Bootwalla MS, Bowen J, Bowlby R, Brooks D, Cherniack AD, Chin L, Cho J, Chudamani S, Ciriello G, Davidsen T, Demchok JA, Dennison JB, Ding L, Felau I, Ferguson ML, Frazer S, Gabriel SB, Gao JJ, Gastier-Foster JM, Gatza ML, Gehlenborg N, Gerken M, Getz G, Gibson WJ, Hayes DN, Heiman DI, Hoadley KA, Holbrook A, Holt RA, Hoyle AP, Hu H, Huang M, Hutter CM, Hwang ES, Jefferys SR, Jones SJM, Ju Z, Kim J, Lai PH, Laird PW, Lawrence MS, Leraas KM, Lichtenberg TM, Lin P, Ling S, Liu J, Liu W, Lolla L, Lu Y, Ma Y, Maglinte DT, Mardis E, Marks J, Marra MA, McAllister C, McLellan M, Meng S, Meyerson M, Mills GB, Moore RA, Mose LE, Mungall AJ, Murray BA, Naresh R, Noble MS, Oesterreich S, Olopade O, Parker JS, Perou CM, Pihl T, Saksena G, Schumacher SE, Shaw KRM, Ramirez NC, Rathmell WK, Rhie SK, Roach J, Robertson AG, Saksena G, Sander C, Schein JE, Schultz N, Shen H, Sheth M, Shi Y, Shih J, Shelley CS, Shriver C, Simons JV, Sofia HJ, Soloway MG, Sougnez C, Sun C, Tarnuzzer R, Tiezzi DG, van den Berg DJ, Voet D, Wan Y, Wang Z, Weinstein JN, Weisenberger DJ, Wilkerson MD, Wilson R, Wise L, Wiznerowicz M, Wu J, Wu Y, Yang L, Yau C, Zack TI, Zenklusen JC, Zhang H, Zhang J, Zmuda E. Comprehensive molecular portraits of invasive lobular breast cancer. Cell. 2015;163(2):506–519. doi: 10.1016/j.cell.2015.09.033. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
