

Challenging Assumptions of Outcomes and Costs Comparing Peritoneal and Hemodialysis
- PMID: 34711359
- PMCID: PMC8562882
- DOI: 10.1016/j.jval.2021.05.017
Challenging Assumptions of Outcomes and Costs Comparing Peritoneal and Hemodialysis
Abstract
Objectives: Policy makers have suggested increasing peritoneal dialysis (PD) would improve end-stage kidney disease (ESKD) outcomes and reduce Medicare spending compared with hemodialysis (HD). We compared mortality, hospitalizations, and Medicare spending between PD and HD among uninsured adults with incident ESKD.
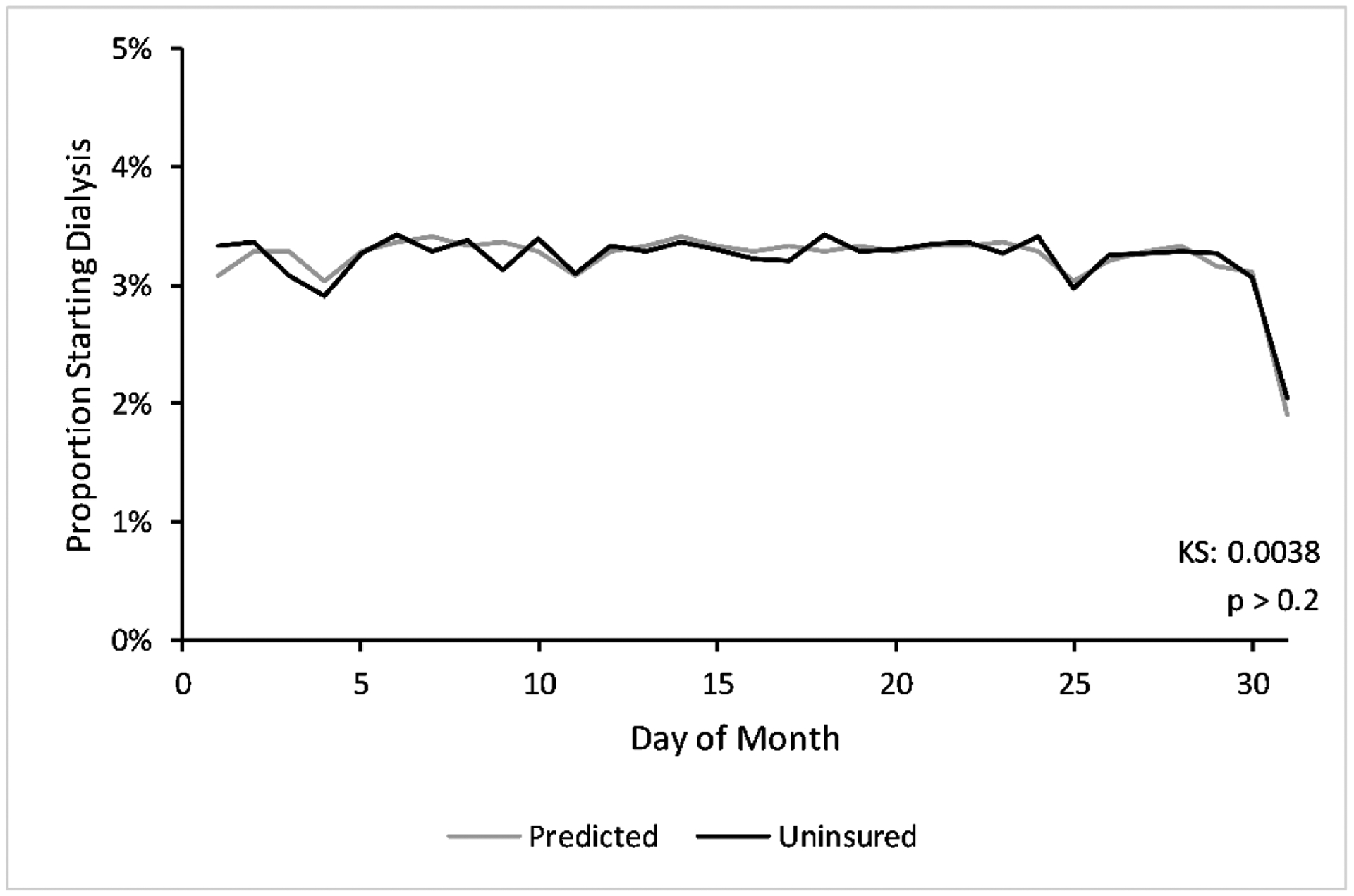
Methods: Using an instrumental variable design, we exploited a natural experiment encouraging PD among the uninsured. Uninsured patients usually receive Medicare at dialysis month 4. For those initiating PD, Medicare covers the first 3 dialysis months, including predialysis services in the calendar month when dialysis started. Starting dialysis later in a calendar month increases predialysis coverage that is essential for PD catheter placements. The policy encourages PD incrementally when ESKD develops later in the month. Dialysis start day appears to be unrelated to patient characteristics and effectively "randomizes patients" to dialysis modality, mitigating selection bias.
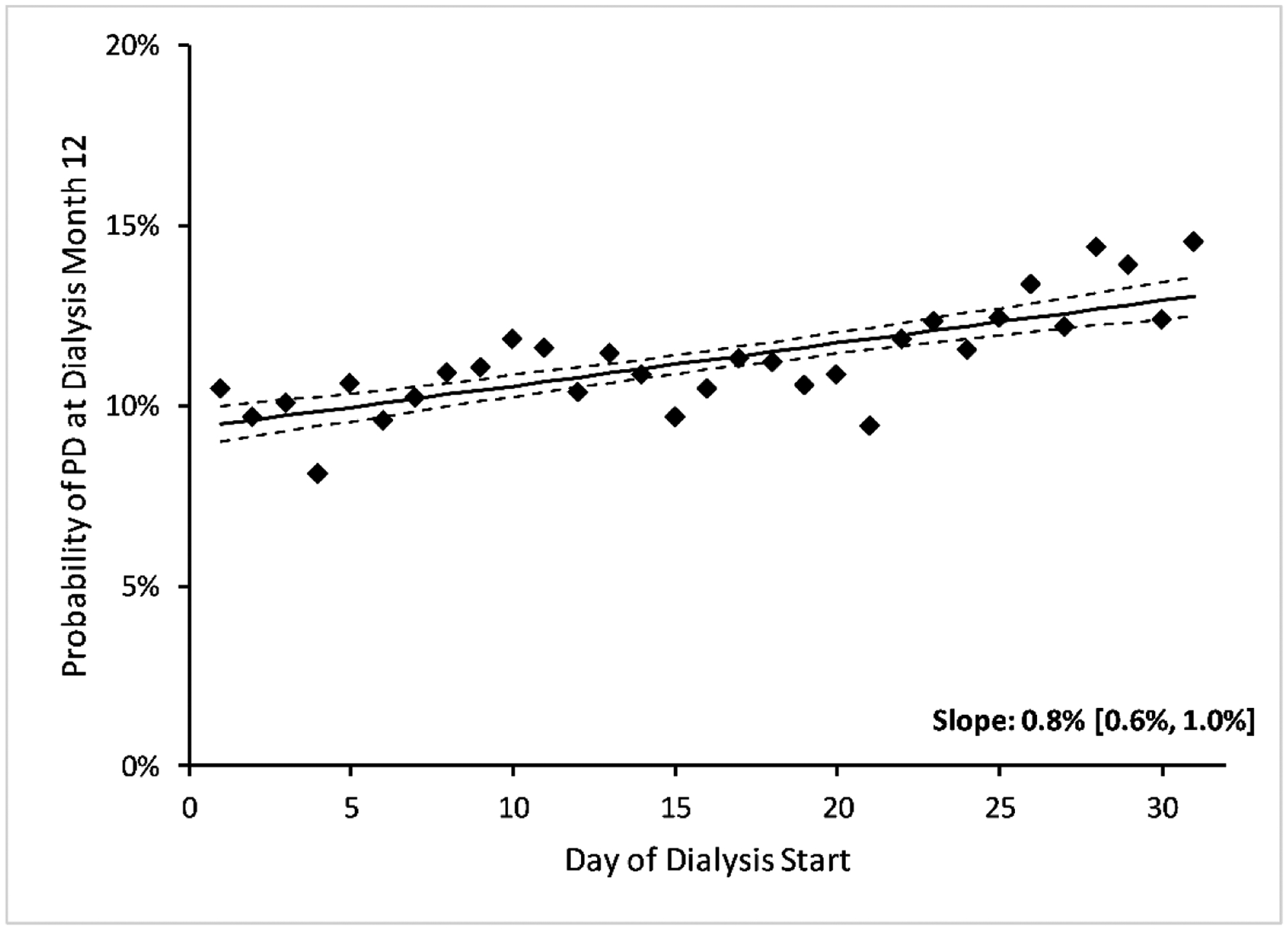
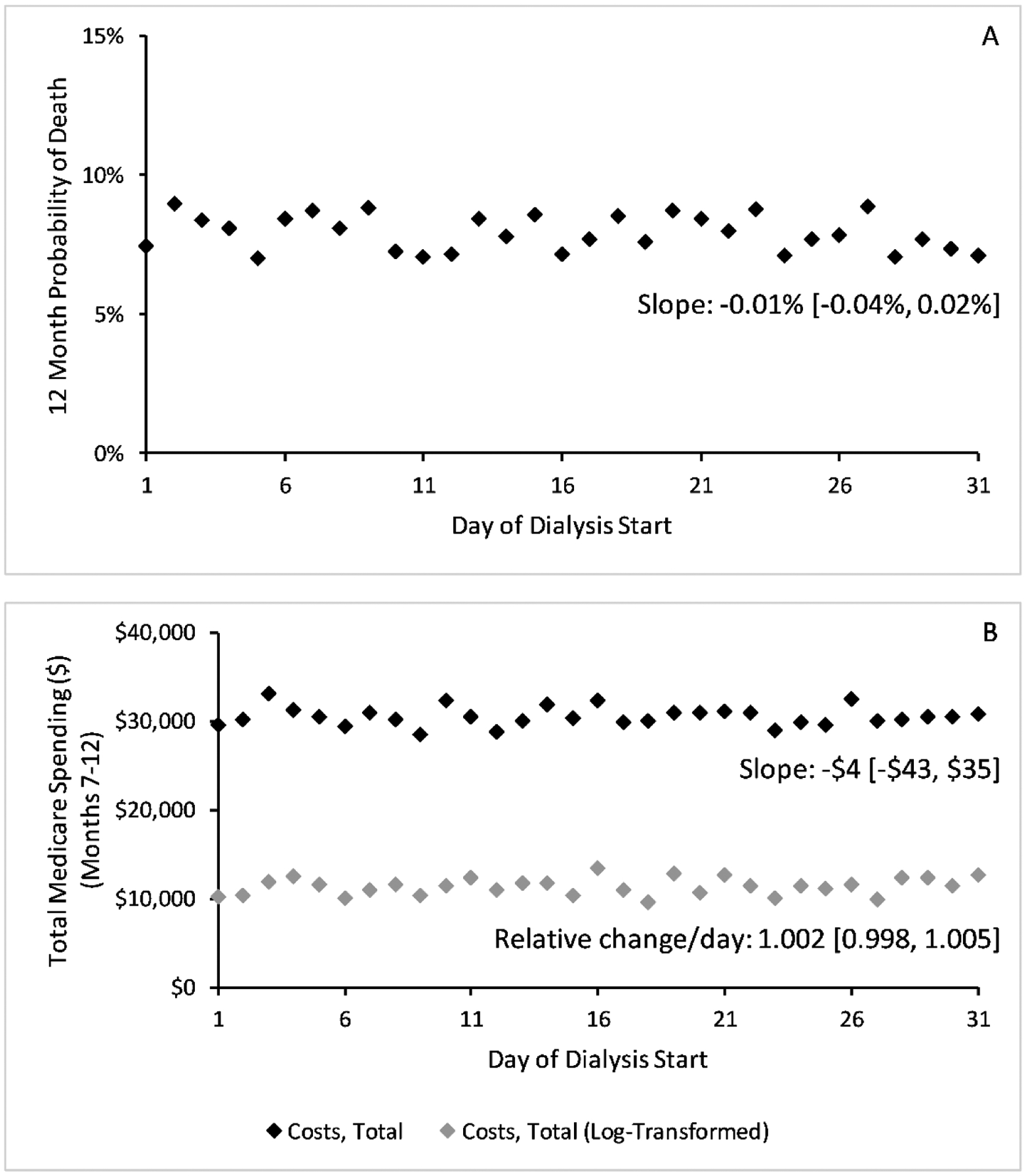
Results: Starting dialysis later in the month was associated with an increased PD uptake: every week later in the month was associated with an absolute increase of 0.8% (95% confidence interval [CI] 0.6%-0.9%) at dialysis day 1 and 0.5% (95% CI 0.3%-0.7%) at dialysis month 12. We observed no significant absolute difference between PD and HD for 12-month mortality (-0.9%, 95% CI -3.3% to 0.8%), hospitalizations during months 7 to 12 (-0.05, 95% CI -0.20 to 0.07), and Medicare spending during months 7 to 12 (-$702, 95% CI -$4004 to $2909).
Conclusions: In an instrumental variable analysis, PD did not result in improved outcomes or lower costs than HD.
Keywords: costs; hemodialysis; instrumental variable; mortality; peritoneal dialysis.
Copyright © 2021 ISPOR–The Professional Society for Health Economics and Outcomes Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- United States Renal Data System. 2019 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2019. Accessed May 7, 2020. https://usrds.org/2019/view/Default.aspx
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
