

The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: a multicenter randomized trial
- PMID: 34711976
- PMCID: PMC8604725
- DOI: 10.1038/s41591-021-01536-x
The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: a multicenter randomized trial
Abstract
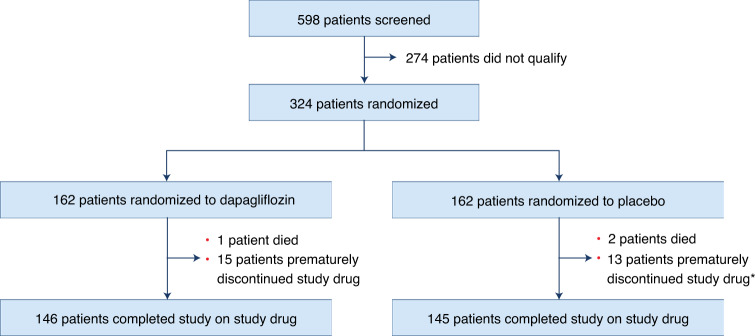
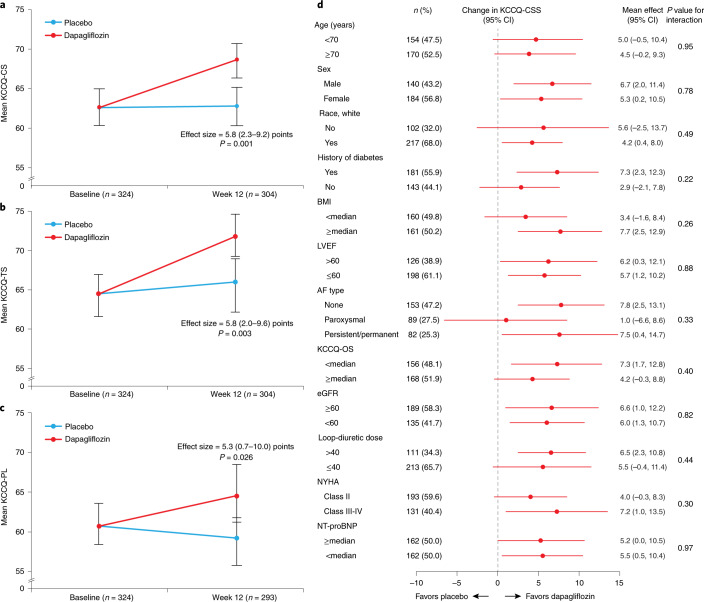
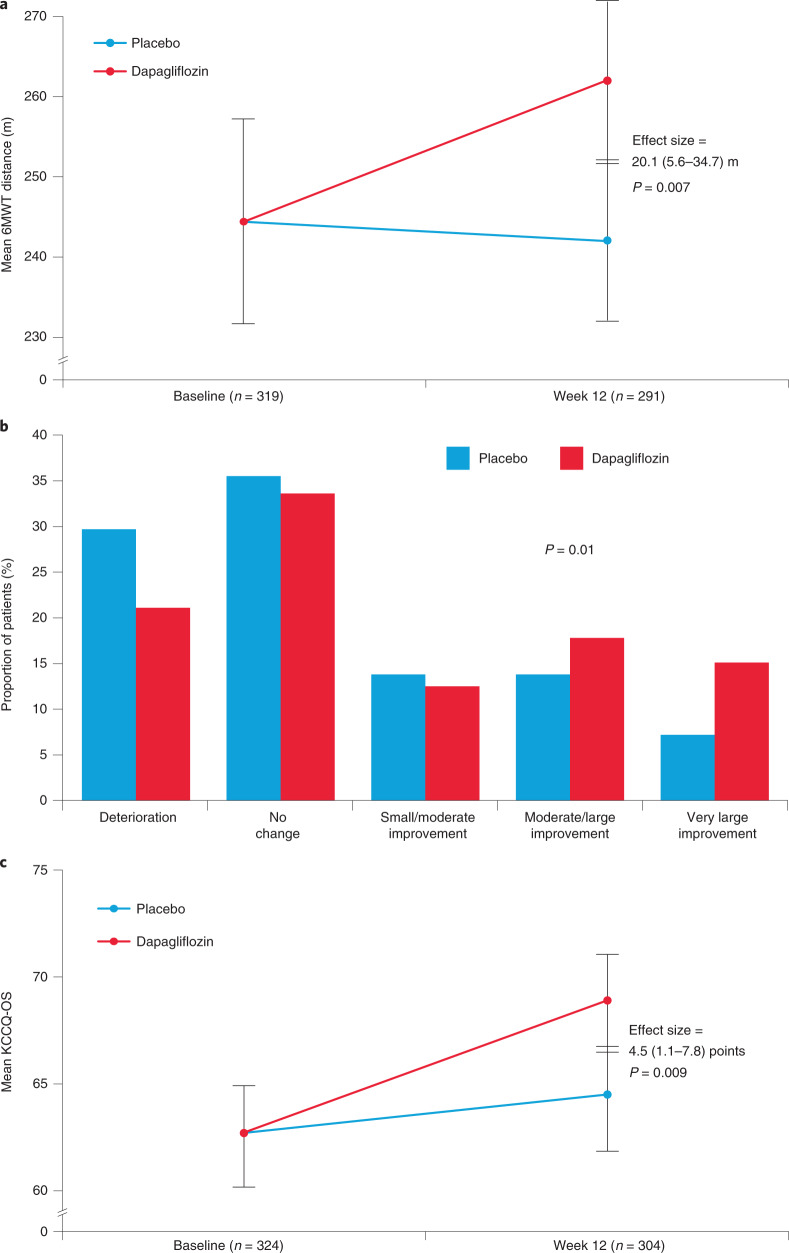
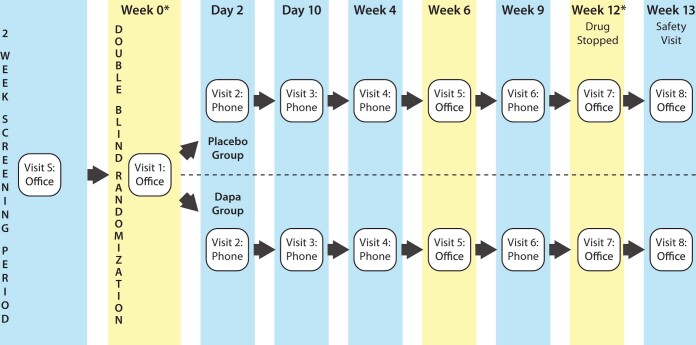
Patients with heart failure and preserved ejection fraction (HFpEF) have a high burden of symptoms and functional limitations, and have a poor quality of life. By targeting cardiometabolic abmormalities, sodium glucose cotransporter 2 (SGLT2) inhibitors may improve these impairments. In this multicenter, randomized trial of patients with HFpEF (NCT03030235), we evaluated whether the SGLT2 inhibitor dapagliflozin improves the primary endpoint of Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CS), a measure of heart failure-related health status, at 12 weeks after treatment initiation. Secondary endpoints included the 6-minute walk test (6MWT), KCCQ Overall Summary Score (KCCQ-OS), clinically meaningful changes in KCCQ-CS and -OS, and changes in weight, natriuretic peptides, glycated hemoglobin and systolic blood pressure. In total, 324 patients were randomized to dapagliflozin or placebo. Dapagliflozin improved KCCQ-CS (effect size, 5.8 points (95% confidence interval (CI) 2.3-9.2, P = 0.001), meeting the predefined primary endpoint, due to improvements in both KCCQ total symptom score (KCCQ-TS) (5.8 points (95% CI 2.0-9.6, P = 0.003)) and physical limitations scores (5.3 points (95% CI 0.7-10.0, P = 0.026)). Dapagliflozin also improved 6MWT (mean effect size of 20.1 m (95% CI 5.6-34.7, P = 0.007)), KCCQ-OS (4.5 points (95% CI 1.1-7.8, P = 0.009)), proportion of participants with 5-point or greater improvements in KCCQ-OS (odds ratio (OR) = 1.73 (95% CI 1.05-2.85, P = 0.03)) and reduced weight (mean effect size, 0.72 kg (95% CI 0.01-1.42, P = 0.046)). There were no significant differences in other secondary endpoints. Adverse events were similar between dapagliflozin and placebo (44 (27.2%) versus 38 (23.5%) patients, respectively). These results indicate that 12 weeks of dapagliflozin treatment significantly improved patient-reported symptoms, physical limitations and exercise function and was well tolerated in chronic HFpEF.
© 2021. The Author(s).
Conflict of interest statement
M.N.K. has received research grants from AstraZeneca and Boehringer Ingelheim and is a consultant and/or advisory board member for Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Esperion Therapeutics, Janssen, Merck (Diabetes and Cardiovascular), Novo Nordisk, Sanofi and Vifor Pharma. M.E.N. is a consultant to Amgen and Roche Vifor and has received speaking honoraria from Abbott. B.A.B. has grant/research Support from National Institutes of Health (NIH)/NHLBI, Axon, AstraZeneca, Corvia, Medtronic, GlaxoSmithKline, Mesoblast, Novartis and Tenax Therapeutics and consulting/advisory board with Actelion, Amgen, Aria, Boehringer Ingelheim, Edwards Lifesciences, Eli Lilly, Imbria, Janssen, Merck, Novo Nordisk, NGMBio, ShouTi and VADovations. D.W.K. has received honoraria as a consultant for Bayer, Merck, Medtronic, Relypsa, Merck, Corvia Medical, Boehringer Ingelheim, NovoNordisk, AstraZeneca and Novartis, grant funding from Novartis, Bayer, NovoNordisk and AstraZeneca and has stock ownership in Gilead Sciences. S.J.S. has research grants from the National Institutes of Health (nos. R01 HL107577, R01 HL127028, R01 HL140731, R01 HL149423), Actelion, AstraZeneca, Corvia, Novartis and Pfizer and consulting fees from Abbott, Actelion, AstraZeneca, Amgen, Aria CV, Axon Therapies, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cardiora, CVRx, Cytokinetics, Edwards Lifesciences, Eidos, Eisai, Imara, Impulse Dynamics, Intellia, Ionis, Ironwood, Lilly, Merck, MyoKardia, Novartis, Novo Nordisk, Pfizer, Prothena, Regeneron, Rivus, Sanofi, Shifamed, Tenax, Tenaya and United Therapeutics. G.U. is partly supported by research grants from the NIH/NATS (no. UL1 TR002378) from the Clinical and Translational Science Award program, and NIH/NIDDK (no. 1P30DK111024-01) from NIH and National Center for Research Resources and has received unrestricted research support for research studies (to Emory University) from Novo Nordisk, AstraZeneca and Dexcom Inc. K.S. is an advisory board member and consultant for Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cytokinetics, Janssen, Novartis and NovoNordisk and receives honoraria. S.S.K. receives funding from AHA (no. 19TPA34890060) and NIH (no. 1R01HL159250). S.-P.C. is a consultant for Edwards Life Sciences and has received speaking honoraria from Abbott. M.K.K. is an advisory board member for Bayer, Abiomed and CareDx. E.S.S. receives research support from, and is a consultant and speaker for, NovoNordisk, is a consultant and speaker for Boehringer Ingelheim and is a consultant and speaker for Eli Lilly. G.D.L. acknowledges research funding from NIH (nos. R01-HL 151841, R01-HL131029, R01-HL159514), American Heart Association (no. 15GPSGC-24800006) and Amgen, Cytokinetics, Applied Therapeutics, AstraZeneca and Sonivie in relation to projects that are distinct from this work; has received honoraria for advisory boards outside of the current study from Pfizer, Merck, Boehringer Ingelheim, Novartis, American Regent, Cyclerion, Cytokinetics and Amgen; and receives royalties from UpToDate for scientific content authorship related to exercise physiology. An AstraZeneca research grant to M.N.K. provided the funding for the PRESERVED-HF trial. None of the other relationships are relevant to the content of this paper. S.L.W., F.T., Y.K., A.O.M., T.K., S.L., C.H.C., L.C., J.J.R., R.A.G., M.P., S.M.J., B.S.C. and M.F. declare no competing interests.
Figures
Comment in
-
Lessons from SGLT-2 inhibitors: rethinking endpoints for heart failure studies.Nat Med. 2021 Nov;27(11):1872-1873. doi: 10.1038/s41591-021-01565-6. Nat Med. 2021. PMID: 34764484 No abstract available.
-
Dapagliflozin improves exercise capacity in HFpEF.Nat Rev Cardiol. 2022 Jan;19(1):6. doi: 10.1038/s41569-021-00650-0. Nat Rev Cardiol. 2022. PMID: 34815543 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
