

Prognostic Nomogram for Liver Metastatic Colon Cancer Based on Histological Type, Tumor Differentiation, and Tumor Deposit: A TRIPOD Compliant Large-Scale Survival Study
- PMID: 34712601
- PMCID: PMC8546254
- DOI: 10.3389/fonc.2021.604882
Prognostic Nomogram for Liver Metastatic Colon Cancer Based on Histological Type, Tumor Differentiation, and Tumor Deposit: A TRIPOD Compliant Large-Scale Survival Study
Abstract
Objective: A proportional hazard model was applied to develop a large-scale prognostic model and nomogram incorporating clinicopathological characteristics, histological type, tumor differentiation grade, and tumor deposit count to provide clinicians and patients diagnosed with colon cancer liver metastases (CLM) a more comprehensive and practical outcome measure.
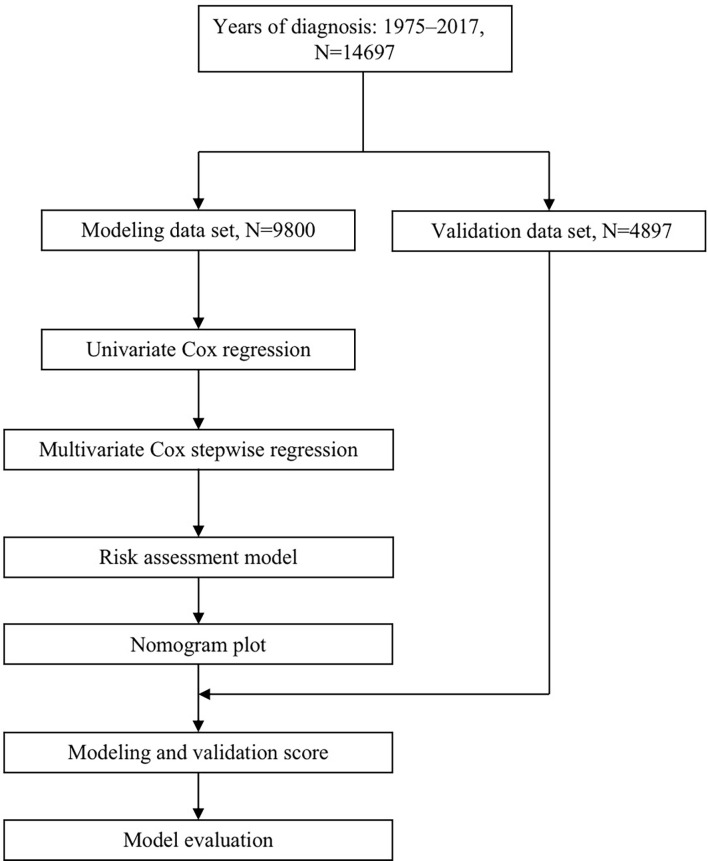
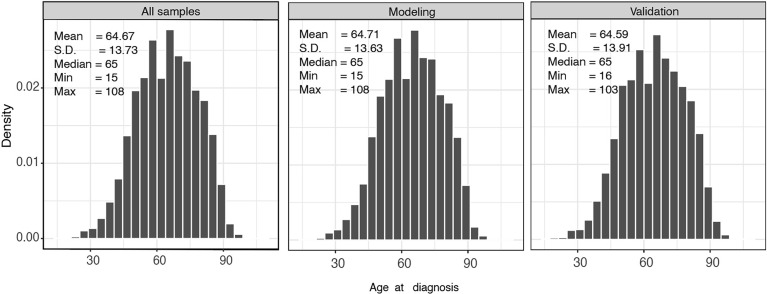
Methods: Using the Transparent Reporting of multivariable prediction models for individual Prognosis or Diagnosis (TRIPOD) guidelines, this study identified 14,697 patients diagnosed with CLM from 1975 to 2017 in the Surveillance, Epidemiology, and End Results (SEER) 21 registry database. Patients were divided into a modeling group (n=9800), an internal validation group (n=4897) using computerized randomization. An independent external validation cohort (n=60) was obtained. Univariable and multivariate Cox analyses were performed to identify prognostic predictors for overall survival (OS). Subsequently, the nomogram was constructed, and the verification was undertaken by receiver operating curves (AUC) and calibration curves.
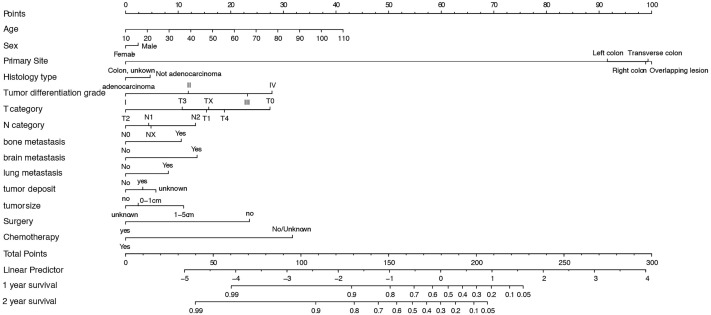
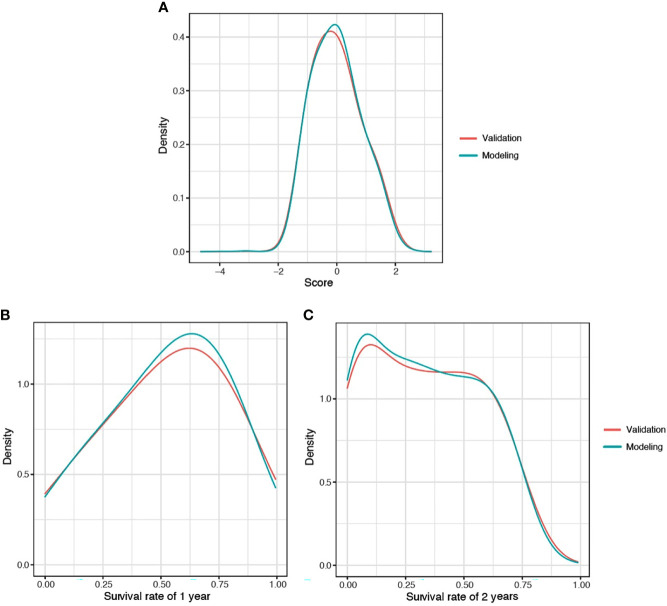
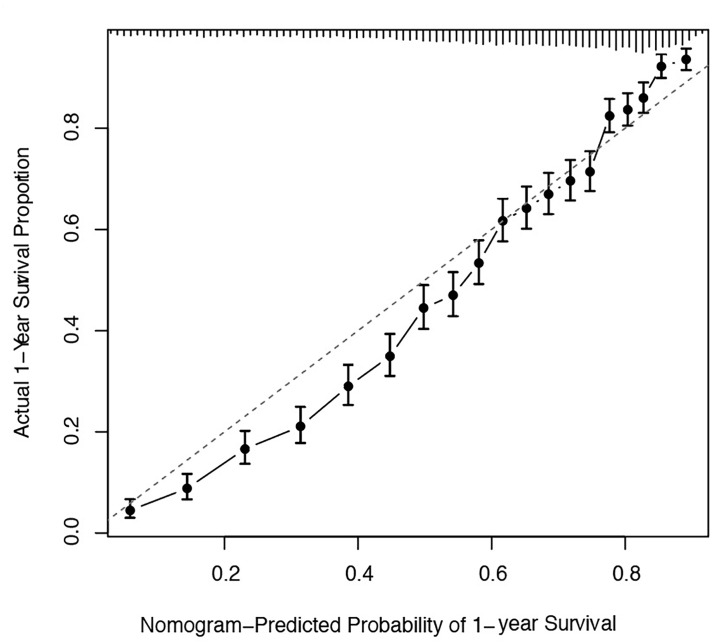
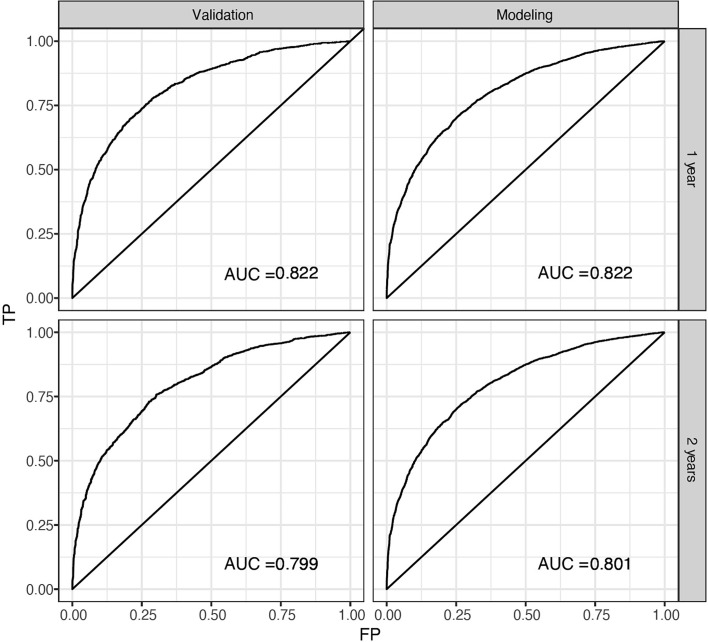
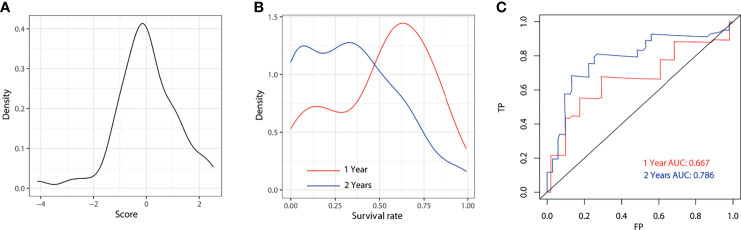
Results: Histological type, tumor differentiation grade, and tumor deposit count were independent prognostic predictors for CLM. The nomogram consisted of age, sex, primary site, T category, N category, metastasis of bone, brain or lung, surgery, and chemotherapy. The model achieved excellent prediction power on both internal (mean AUC=0.811) and external validation (mean AUC=0.727), respectively, which were significantly higher than the American Joint Committee on Cancer (AJCC) TNM system.
Conclusion: This study proposes a prognostic nomogram for predicting 1- and 2-year survival based on histopathological and population-based data of CLM patients developed using TRIPOD guidelines. Compared with the TNM stage, our nomogram has better consistency and calibration for predicting the OS of CLM patients.
Keywords: colon cancer; database analysis; liver metastasis; nomogram; prognosis model.
Copyright © 2021 Kuai, Zhang, Luo, Li, Li, Zhang, Liu, Yin and Li.
Conflict of interest statement
Authors H-PZ and T-YL were employed by Research and Development Center, Shanghai Applied Protein Technology Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS, et al. . Global Surveillance of Cancer Survival 1995-2009: Analysis of Individual Data for 25,676,887 Patients From 279 Population-Based Registries in 67 Countries (CONCORD-2). Lancet (2015) 385(9972):977–1010. doi: 10.1016/S0140-6736(14)62038-9 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources