

Altered Cytokine Endotoxin Responses in Neonatal Encephalopathy Predict MRI Outcomes
- PMID: 34712631
- PMCID: PMC8547258
- DOI: 10.3389/fped.2021.734540
Altered Cytokine Endotoxin Responses in Neonatal Encephalopathy Predict MRI Outcomes
Abstract
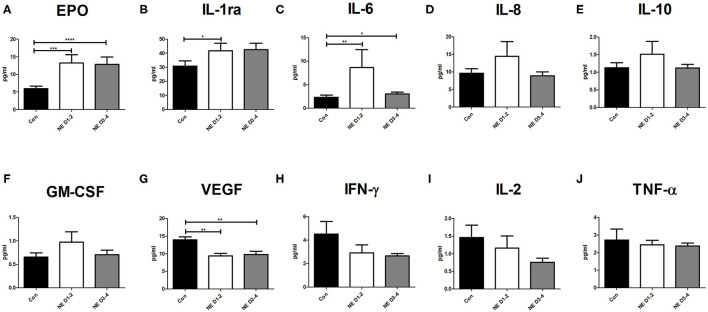
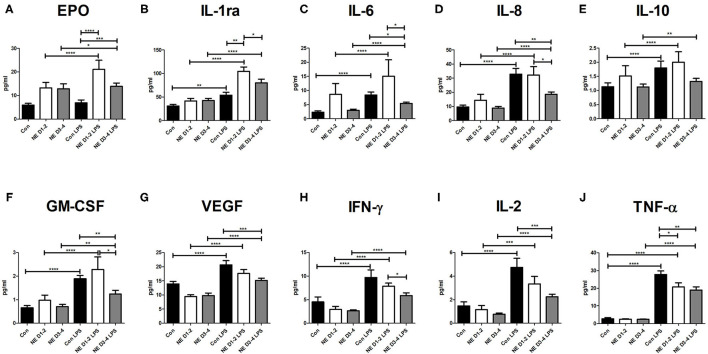
Background: Neonatal encephalopathy (NE) is associated with adverse neurodevelopmental outcome and is linked with systemic inflammation. Pro-inflammatory and anti-inflammatory cytokines are known to play a role in the pathology of NE by activating innate immune cells. Methods: Eighty-seven infants were enrolled including 53 infants with NE of whom 52 received therapeutic hypothermia (TH) and 34 term infant healthy controls (TC). Whole blood sampling was performed in the first 4 days of life, and a 14-spot ELISA Multiplex Cytokine Array was carried out on baseline samples or after stimulation with lipopolysaccharide (LPS) as an additional inflammatory stimulus. The cytokine medians were examined for differences between infants with NE and healthy TC; and then short-term outcomes of Sarnat stage, seizures, and MRI brain were examined within the NE group. The potential of LPS stimulation to predict abnormal MRI was explored using receiver operating characteristic (ROC) curves. Results: At baseline, infants with NE had significantly higher levels of erythropoietin (Epo), interleukin (IL)-6, and IL-1ra and significantly lower vascular endothelial growth factor (VEGF) than had controls. All cytokines were increased after LPS stimulation in infants with NE with an excessive Epo and IL-1ra response than in controls. Infants with NE had lower IL-8, IL-2, IL-6, tumor necrosis factor (TNF)-α, granulocyte-macrophage colony-stimulating factor (GM-CSF), VEGF, and interferon (IFN)-γ than controls had following LPS. GM-CSF and IFN-γ, IL-1β, IL-1ra, and VEGF were higher on days 1-2 in NE infants with abnormal neuroimaging. GM-CSF, IFN-γ, and TNF-α levels with LPS stimulation were different upon stimulation between normal and abnormal neuroimaging. TNF-α is the only strong cytokine predictor both pre- and post-LPS stimulation of abnormal brain imaging. Conclusions: Altered cytokine responses are found in infants with NE vs. controls, and more significant differences are unmasked by the additional stimulus of LPS, which potentially improves the predictive power of these cytokines for the detection of abnormal MRIs. Infants with NE undergoing TH demonstrate both trained immunity and tolerance, and understanding these responses will facilitate adjunctive immunomodulatory treatments.
Keywords: MRI; biomarkers; cytokines; hypoxic-ischaemic encephalopathy; lipopolysaccharide; neonatal encephalopathy; neurodevelopment.
Copyright © 2021 O'Dea, Kelly, McKenna, Strickland, Hurley, Butler, Vavasseur, EL-Khuffash, Miletin, Fallah, White, Wyse and Molloy.
Conflict of interest statement
JB was employed by MSD. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials