

Retrospective Study of Critically Ill COVID-19 Patients With and Without Extracorporeal Membrane Oxygenation Support in Wuhan, China
- PMID: 34712673
- PMCID: PMC8546219
- DOI: 10.3389/fmed.2021.659793
Retrospective Study of Critically Ill COVID-19 Patients With and Without Extracorporeal Membrane Oxygenation Support in Wuhan, China
Abstract
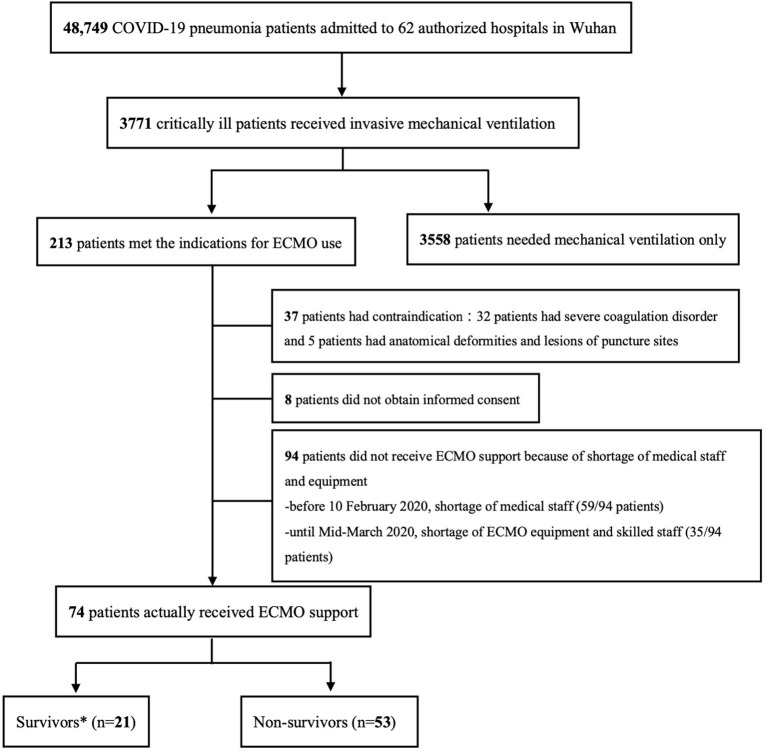
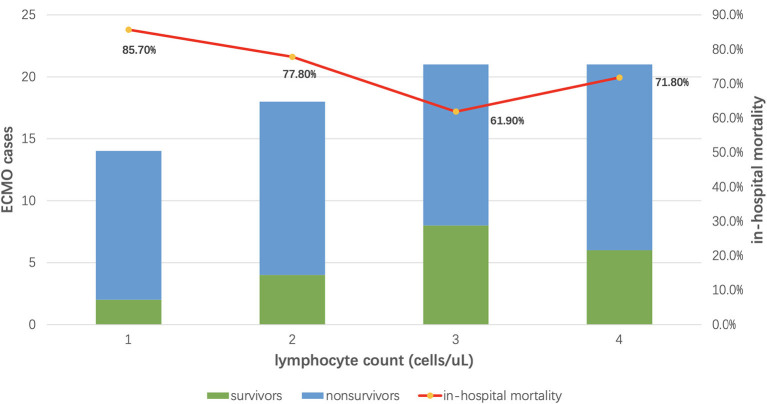
Background: Extracorporeal membrane oxygenation (ECMO) might benefit critically ill COVID-19 patients. But the considerations besides indications guiding ECMO initiation under extreme pressure during the COVID-19 epidemic was not clear. We aimed to analyze the clinical characteristics and in-hospital mortality of severe critically ill COVID-19 patients supported with ECMO and without ECMO, exploring potential parameters for guiding the initiation during the COVID-19 epidemic. Methods: Observational cohort study of all the critically ill patients indicated for ECMO support from January 1 to May 1, 2020, in all 62 authorized hospitals in Wuhan, China. Results: Among the 168 patients enrolled, 74 patients actually received ECMO support and 94 not were analyzed. The in-hospital mortality of the ECMO supported patients was significantly lower than non-ECMO ones (71.6 vs. 85.1%, P = 0.033), but the role of ECMO was affected by patients' age (Logistic regression OR 0.62, P = 0.24). As for the ECMO patients, the median age was 58 (47-66) years old and 62.2% (46/74) were male. The 28-day, 60-day, and 90-day mortality of these ECMO supported patients were 32.4, 68.9, and 74.3% respectively. Patients survived to discharge were younger (49 vs. 62 years, P = 0.042), demonstrated higher lymphocyte count (886 vs. 638 cells/uL, P = 0.022), and better CO2 removal (PaCO2 immediately after ECMO initiation 39.7 vs. 46.9 mmHg, P = 0.041). Age was an independent risk factor for in-hospital mortality of the ECMO supported patients, and a cutoff age of 51 years enabled prediction of in-hospital mortality with a sensitivity of 84.3% and specificity of 55%. The surviving ECMO supported patients had longer ICU and hospital stays (26 vs. 18 days, P = 0.018; 49 vs. 29 days, P = 0.001 respectively), and ECMO procedure was widely carried out after the supplement of medical resources after February 15 (67.6%, 50/74). Conclusions: ECMO might be a benefit for severe critically ill COVID-19 patients at the early stage of epidemic, although the in-hospital mortality was still high. To initiate ECMO therapy under tremendous pressure, patients' age, lymphocyte count, and adequacy of medical resources should be fully considered.
Keywords: COVID-19; SARS-CoV-2; critically ill pneumonia; extracorporeal membrane oxygenation; in-hospital mortality.
Copyright © 2021 Cheng, Ma, Su, Long, Liu, Du, Qiu, Guan, Chen, Kang, Tong, Peng, Shang, Zheng, Li, Pan, Huang, Zhan, Ding, Huang, Yin, Li, Li, Jiang, Hu, Li, Zhou, Jing, Guo and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. CESAR trial collaboration: efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. (2009) 374:1351–63. 10.1016/S0140-6736(09)61069-2 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous