

Attitudes Toward Health, Healthcare, and eHealth of People With a Low Socioeconomic Status: A Community-Based Participatory Approach
- PMID: 34713165
- PMCID: PMC8521920
- DOI: 10.3389/fdgth.2021.690182
Attitudes Toward Health, Healthcare, and eHealth of People With a Low Socioeconomic Status: A Community-Based Participatory Approach
Abstract
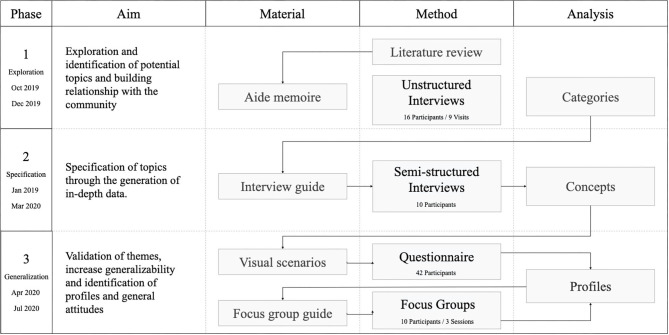
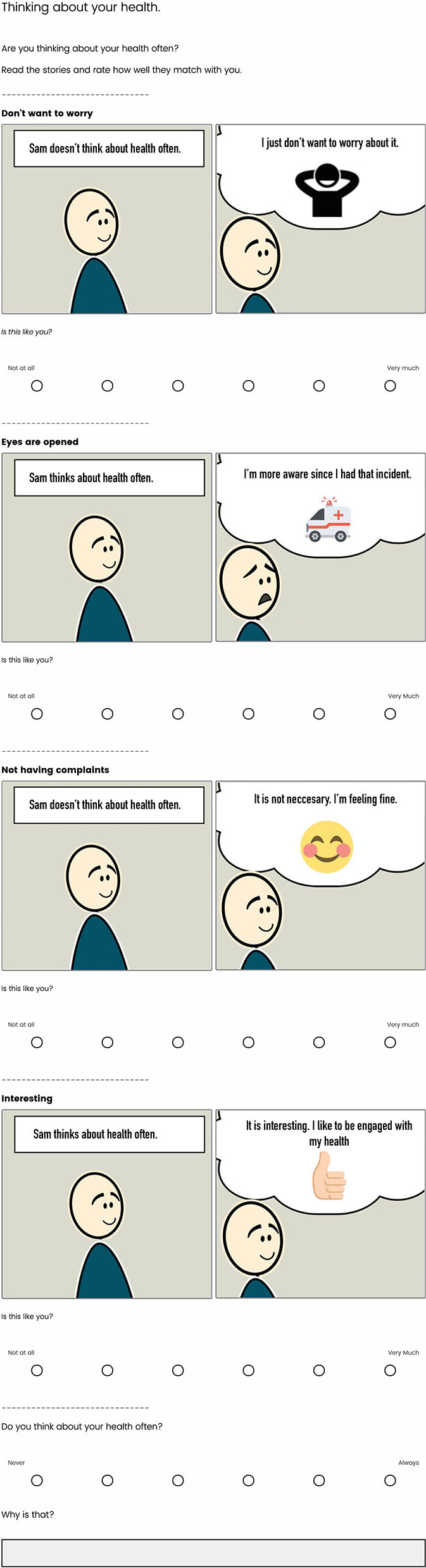
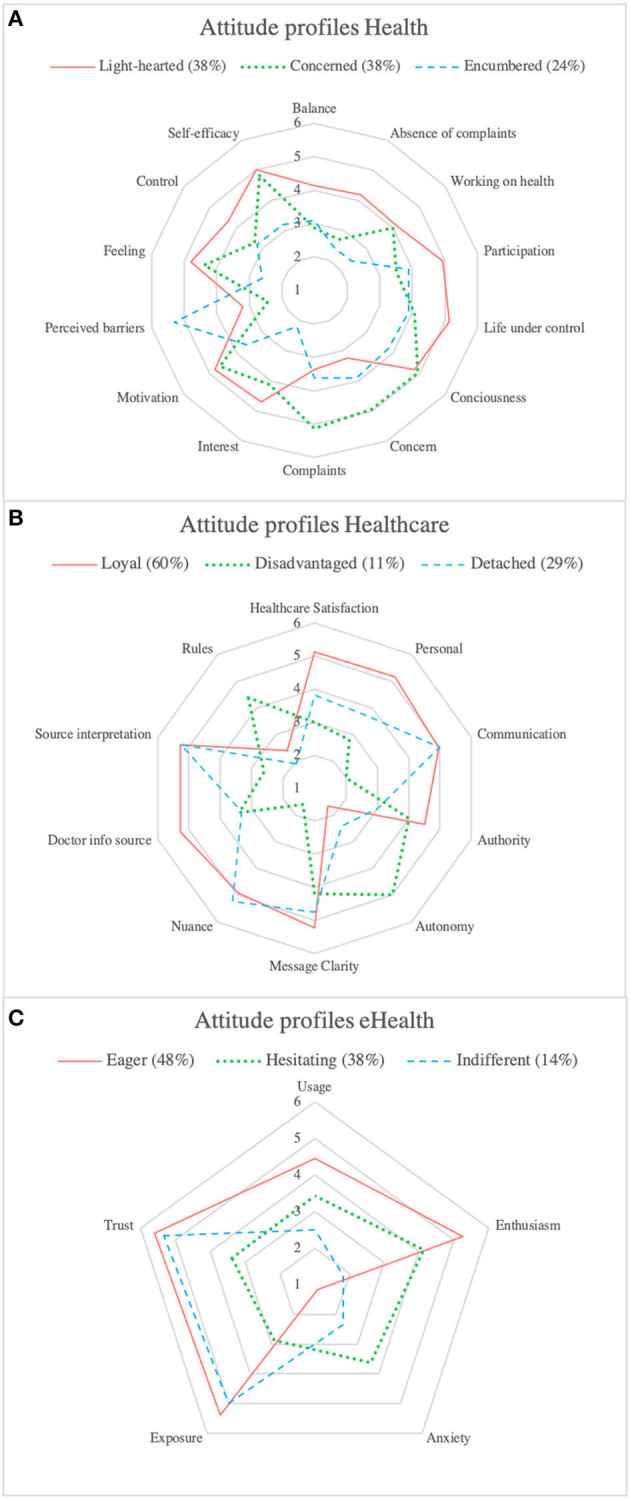
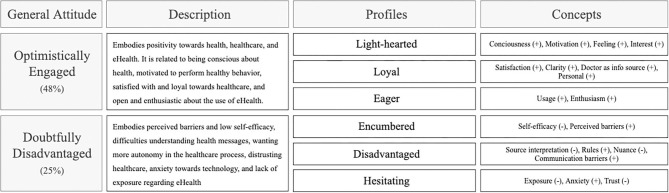
Low socioeconomic status (SES) is associated with a higher prevalence of unhealthy lifestyles compared to a high SES. Health interventions that promote a healthy lifestyle, like eHealth solutions, face limited adoption in low SES groups. To improve the adoption of eHealth interventions, their alignment with the target group's attitudes is crucial. This study investigated the attitudes of people with a low SES toward health, healthcare, and eHealth. We adopted a mixed-method community-based participatory research approach with 23 members of a community center in a low SES neighborhood in the city of Rotterdam, the Netherlands. We conducted a first set of interviews and analyzed these using a grounded theory approach resulting in a group of themes. These basic themes' representative value was validated and refined by an online questionnaire involving a different sample of 43 participants from multiple community centers in the same neighborhood. We executed three focus groups to validate and contextualize the results. We identified two general attitudes based on nine profiles toward health, healthcare, and eHealth. The first general attitude, optimistically engaged, embodied approximately half our sample and involved light-heartedness toward health, loyalty toward healthcare, and eagerness to adopt eHealth. The second general attitude, doubtfully disadvantaged, represented roughly a quarter of our sample and was related to feeling encumbered toward health, feeling disadvantaged within healthcare, and hesitance toward eHealth adoption. The resulting attitudes strengthen the knowledge of the motivation and behavior of people with low SES regarding their health. Our results indicate that negative health attitudes are not as evident as often claimed. Nevertheless, intervention developers should still be mindful of differentiating life situations, motivations, healthcare needs, and eHealth expectations. Based on our findings, we recommend eHealth should fit into the person's daily life, ensure personal communication, be perceived usable and useful, adapt its communication to literacy level and life situation, allow for meaningful self-monitoring and embody self-efficacy enhancing strategies.
Keywords: community-based participatory research; eHealth adoption; eHealth intervention design; health attitudes; health disparities; low socioeconomic status; user profiles.
Copyright © 2021 Faber, Al-Dhahir, Reijnders, Chavannes, Evers, Kraal, van den Berg-Emons and Visch.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources