

Association of Estimated Cardiorespiratory Fitness in Midlife With Cardiometabolic Outcomes and Mortality
- PMID: 34714339
- PMCID: PMC8556623
- DOI: 10.1001/jamanetworkopen.2021.31284
Association of Estimated Cardiorespiratory Fitness in Midlife With Cardiometabolic Outcomes and Mortality
Abstract
Importance: The associations of estimated cardiorespiratory fitness (eCRF) during midlife with subclinical atherosclerosis, arterial stiffness, incident cardiometabolic disease, and mortality are not well understood.
Objective: To examine associations of midlife eCRF with subclinical atherosclerosis, arterial stiffness, incident cardiometabolic disease, and mortality.
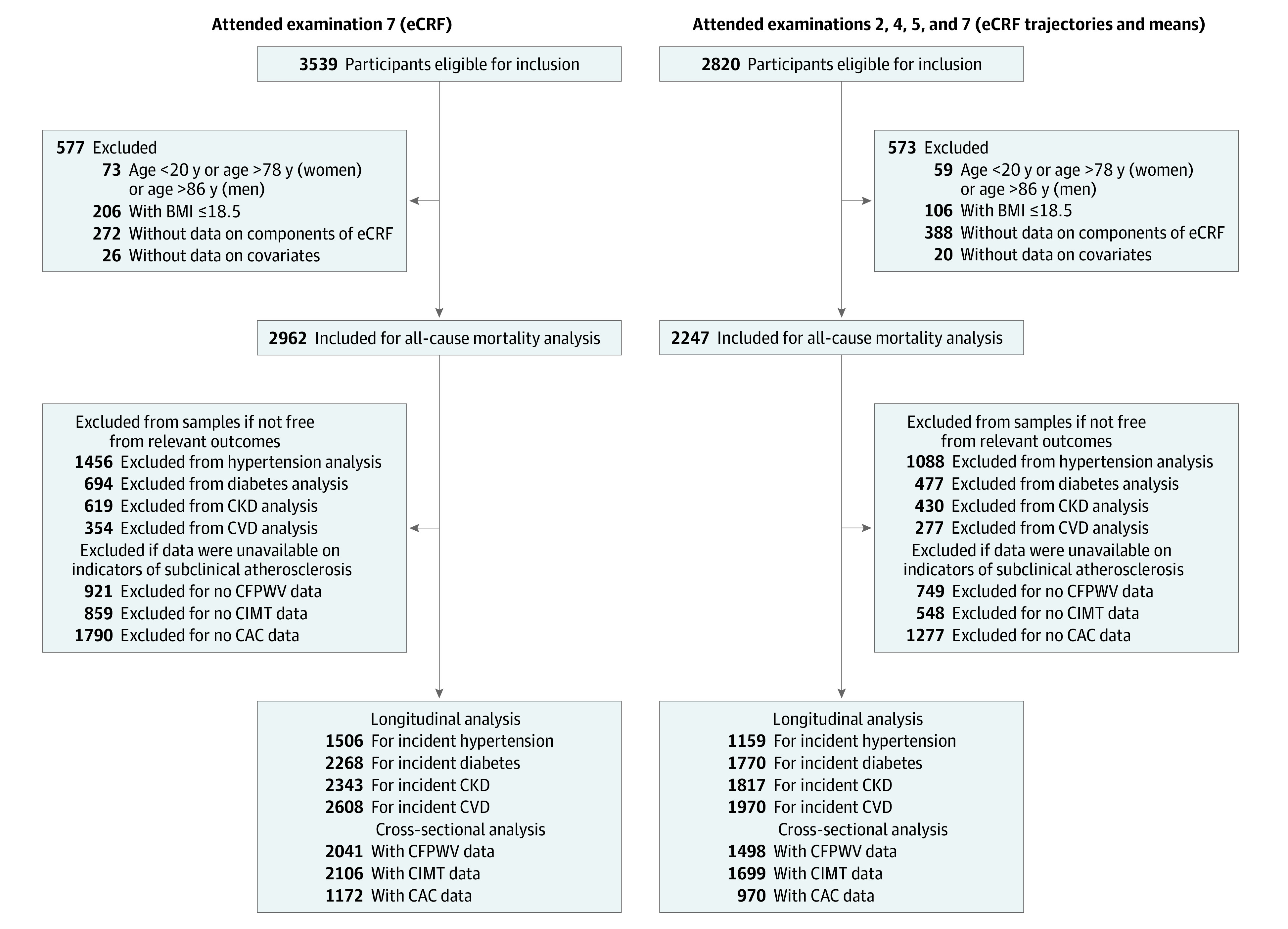
Design, setting, and participants: This cohort study included 2962 participants in the Framingham Study Second Generation (conducted between 1979 and 2001). Data were analyzed from January 2020 to June 2020.
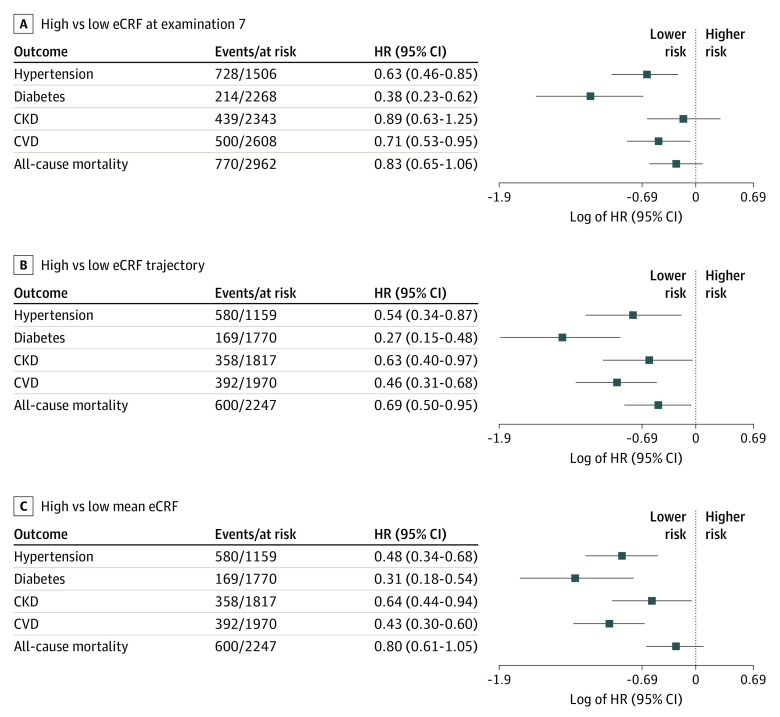
Exposures: eCRF was calculated using sex-specific algorithms (including age, body mass index, waist circumference, physical activity, resting heart rate, and smoking) and was categorized as: (1) tertiles of standardized eCRF at examination cycle 7 (1998 to 2001); (2) tertiles of standardized average eCRF between examination cycles 2 and 7 (1979 to 2001); and (3) eCRF trajectories between examination cycles 2 and 7, with the lowest tertile or trajectory (ie, low eCRF) as referent group.
Main outcomes and measures: Subclinical atherosclerosis (carotid intima-media thickness [CIMT], coronary artery calcium [CAC] score); arterial stiffness (carotid-femoral pulse wave velocity [-1000/CFPWV]); incident hypertension, diabetes, chronic kidney disease (CKD), cardiovascular disease (CVD), and mortality after examination cycle 7.
Results: A total of 2962 participants were included in this cohort study (mean [SD] age, 61.5 [9.2] years; 1562 [52.7%] women). The number of events or participants at risk after examination cycle 7 (at a mean follow-up of 15 years) was 728 of 1506 for hypertension, 214 of 2268 for diabetes, 439 of 2343 for CKD, 500 of 2608 for CVD, and 770 of 2962 for mortality. Compared with the low eCRF reference value, high single examination eCRF was associated with lower CFPWV (β [SE], -11.13 [1.33] ms/m) and CIMT (β [SE], -0.12 [0.05] mm), and lower risk of hypertension (hazard ratio [HR], 0.63; 95% CI, 0.46-0.85), diabetes (HR, 0.38; 95% CI, 0.23-0.62), and CVD (HR, 0.71; 95% CI, 0.53-0.95), although it was not associated with CKD or mortality. Similarly, compared with the low eCRF reference, high eCRF trajectories and mean eCRF were associated with lower CFPWV (β [SE], -11.85 [1.89] ms/m and -10.36 [1.54] ms/m), CIMT (β [SE], -0.19 [0.06] mm and -0.15 [0.05] mm), CAC scores (β [SE], -0.67 [0.25] AU and -0.63 [0.20] AU), and lower risk of hypertension (HR, 0.54; 95% CI, 0.34-0.87 and HR, 0.48; 95% CI, 0.34-0.68), diabetes (HR, 0.27; 95% CI, 0.15-0.48 and HR, 0.31; 95% CI, 0.18-0.54), CKD (HR, 0.63; 95% CI, 0.40-0.97 and HR, 0.64; 95% CI, 0.44-0.94), and CVD (HR, 0.46; 95% CI, 0.31-0.68 and HR, 0.43; 95% CI, 0.30-0.60). Compared with the reference value, a high eCRF trajectory was associated with lower risk of mortality (HR, 0.69; 95% CI, 0.50-0.95).
Conclusions and relevance: In this cohort study, higher midlife eCRF was associated with lower burdens of subclinical atherosclerosis and vascular stiffness, and with a lower risk of hypertension, diabetes, chronic kidney disease, cardiovascular disease, and mortality. These findings suggest that midlife eCRF may serve as a prognostic marker for subclinical atherosclerosis, arterial stiffness, cardiometabolic health, and mortality in later life.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
