

Treatment of multiple huge liver cysts in a hybrid operating room: a case report
- PMID: 34714449
- PMCID: PMC8556466
- DOI: 10.1186/s40792-021-01320-6
Treatment of multiple huge liver cysts in a hybrid operating room: a case report
Abstract
Background: Liver cysts are common, with most cases being asymptomatic. In symptomatic cases, the disease is amenable to treatment. However, huge or multiple liver cysts with vascular narrowing and associated systemic symptoms are extremely rare. Furthermore, the performance of a reliable and effective surgery in such cases remains a major problem. Here, we report a case of multiple giant liver cysts with impaired blood flow surgically treated in a hybrid operating room.
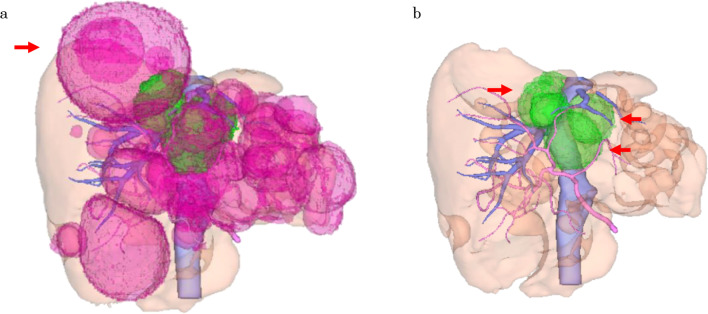
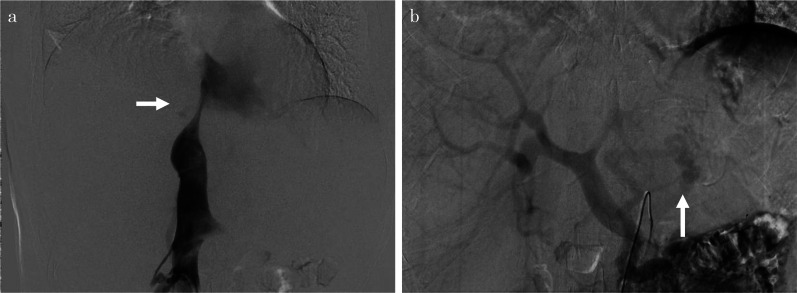
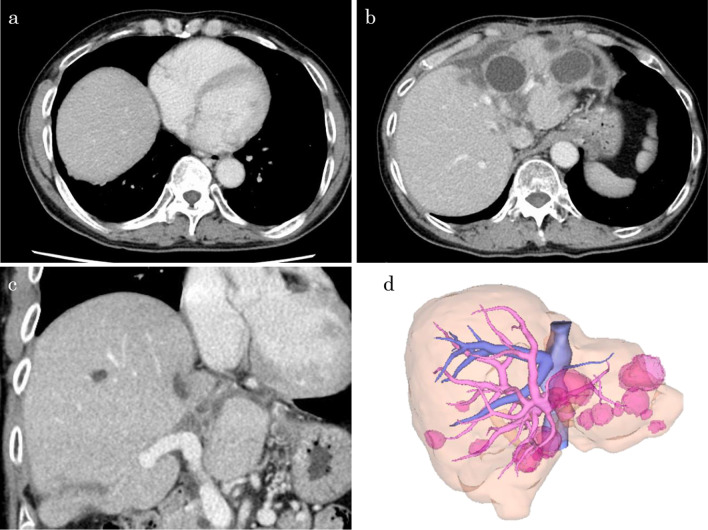
Case presentation: A 73-year-old male presented to a previous doctor with leg edema and dyspnea on exertion; computed tomography revealed that the cause complaint was right lung and heart compression and inferior vena cava (IVC) stenosis due to huge liver cysts in the caudal lobe. The patient was referred to our hospital because of disease recurrence despite percutaneous aspiration of the cyst. Multiple liver cysts were observed in addition to the drained cysts, two of which were located on both sides of the IVC and caused IVC stenosis. We performed open surgery for the liver cysts and used the hybrid operating room for intraoperative IVC angiography and measuring the hepatic vein and portal vein (PV) pressure. We performed unroofing of the hepatic cyst and cauterization of the cyst wall on the hepatic side. Angiography was performed before and after unroofing of the liver cysts, and IVC stenosis release was confirmed. IVC pressure measured at the peripheral side of the stenosis and PV pressures were continuously measured during surgery and were confirmed to have decreased during the opening of the liver cysts. The patient had a good postoperative course and was discharged on the 10th postoperative day. No recurrence was observed 6 months postoperatively.
Conclusions: Cyst unroofing surgery using angiography in a hybrid operating room is a useful treatment for deep hepatic lesions in that vascular stenosis improvement can be intraoperatively confirmed. Moreover, in cases wherein the cyst compresses the vasculature, intraoperative monitoring of IVC and PV pressures can be used to prove that the liver cyst is hemodynamically involved.
Keywords: Angiography; Hepatic cystotomy; Huge liver cysts; Hybrid operating room; Unroofing.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Kashiwagi H, Kumagai K, Nozue M. Single incision laparoscopic surgery for a life-threatening, cyst of liver. Tokai J Exp Clin Med. 2011;36(1):13–16. - PubMed
LinkOut - more resources
Full Text Sources
