

Lack of CD8+ T cell effector differentiation during priming mediates checkpoint blockade resistance in non-small cell lung cancer
- PMID: 34714687
- PMCID: PMC10786005
- DOI: 10.1126/sciimmunol.abi8800
Lack of CD8+ T cell effector differentiation during priming mediates checkpoint blockade resistance in non-small cell lung cancer
Abstract
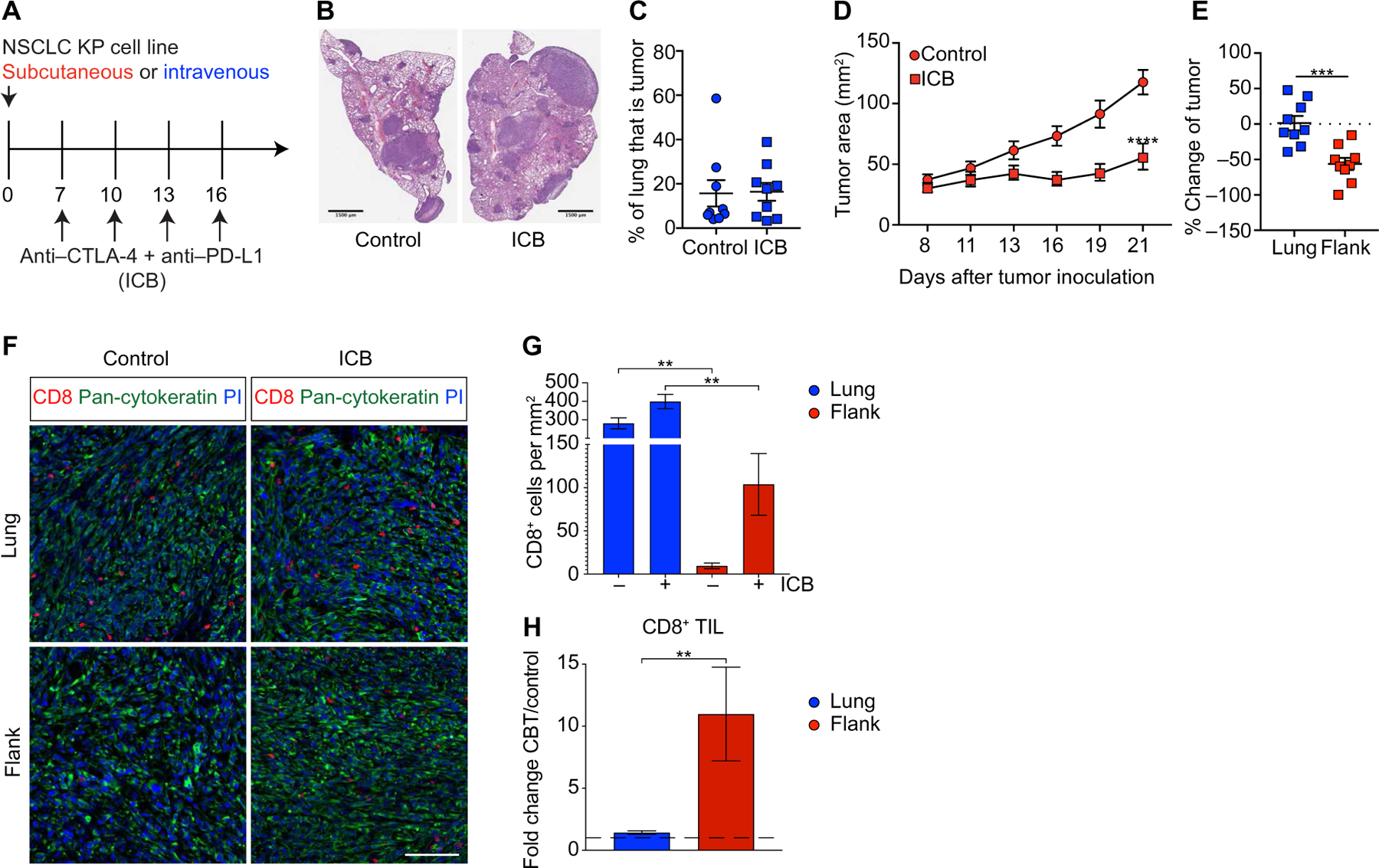
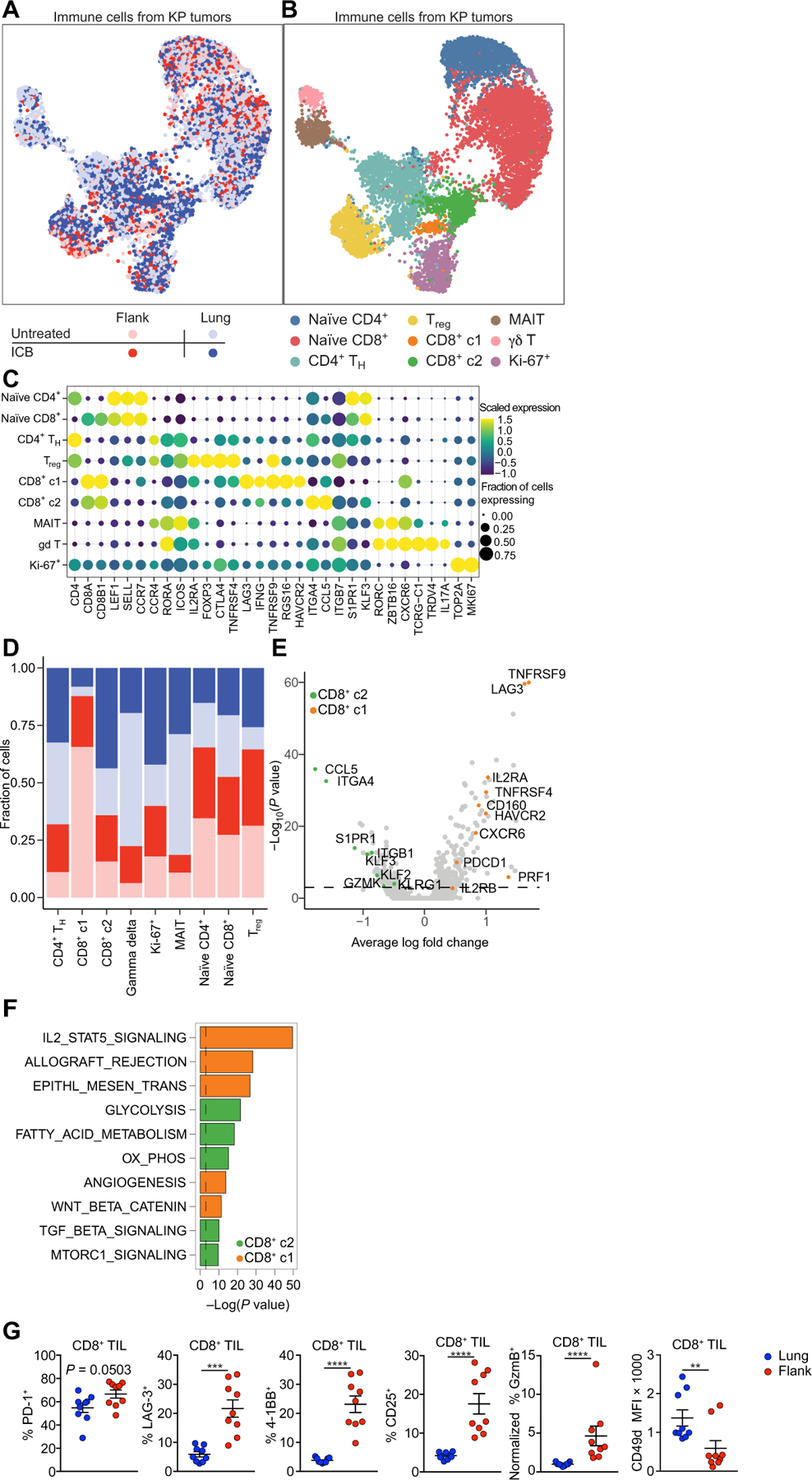
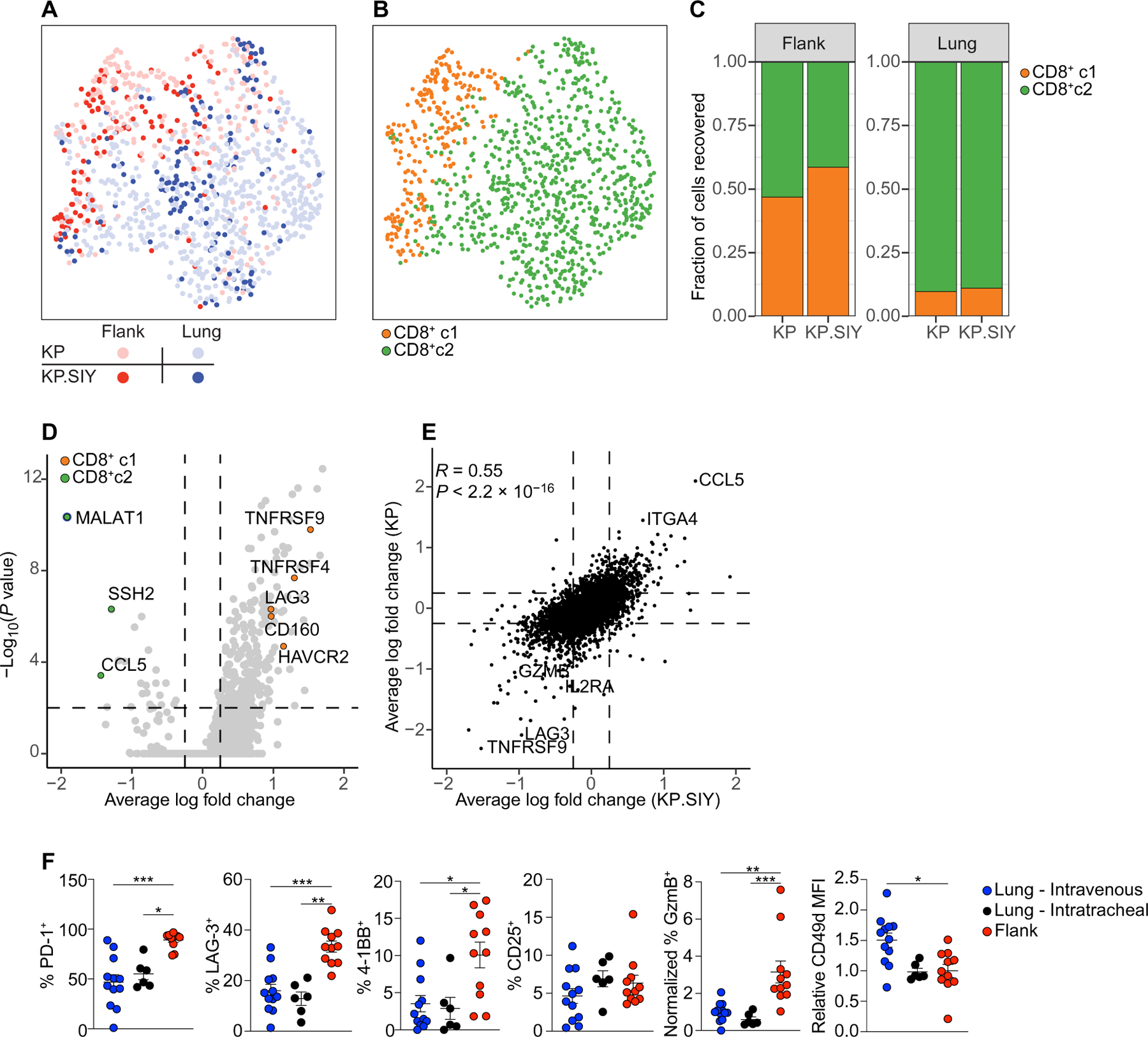
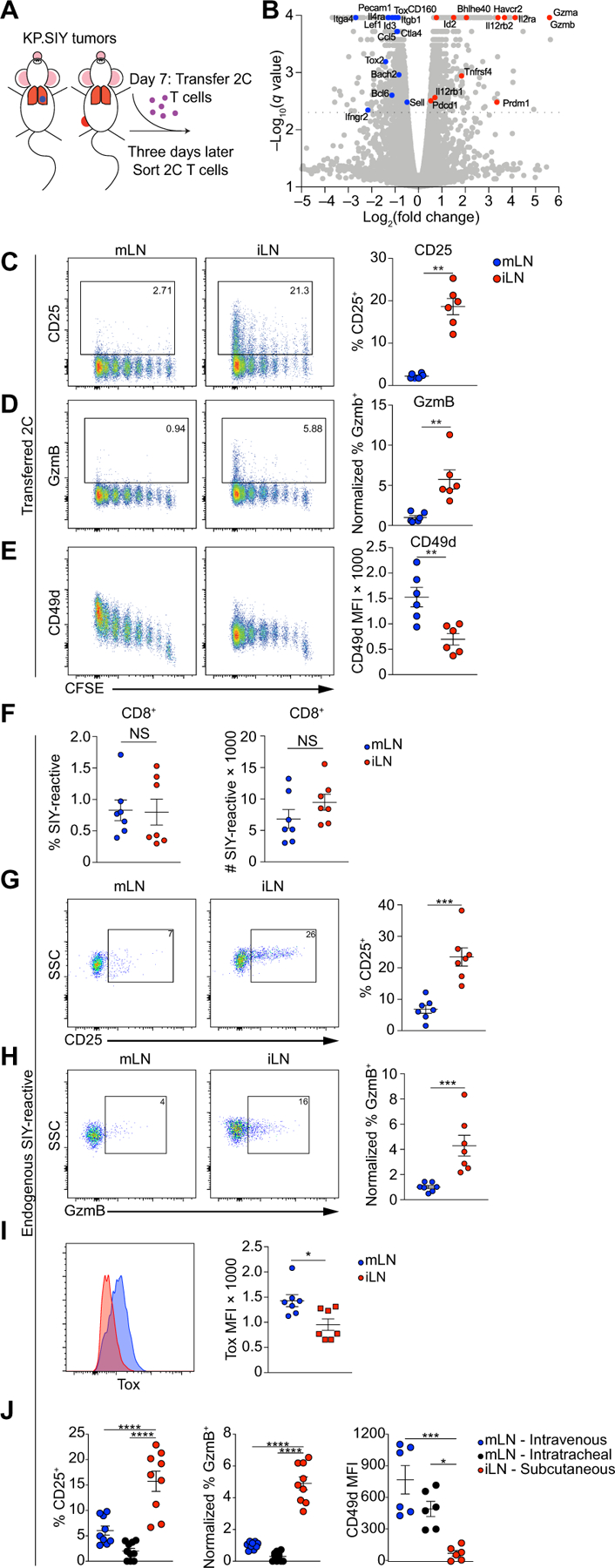
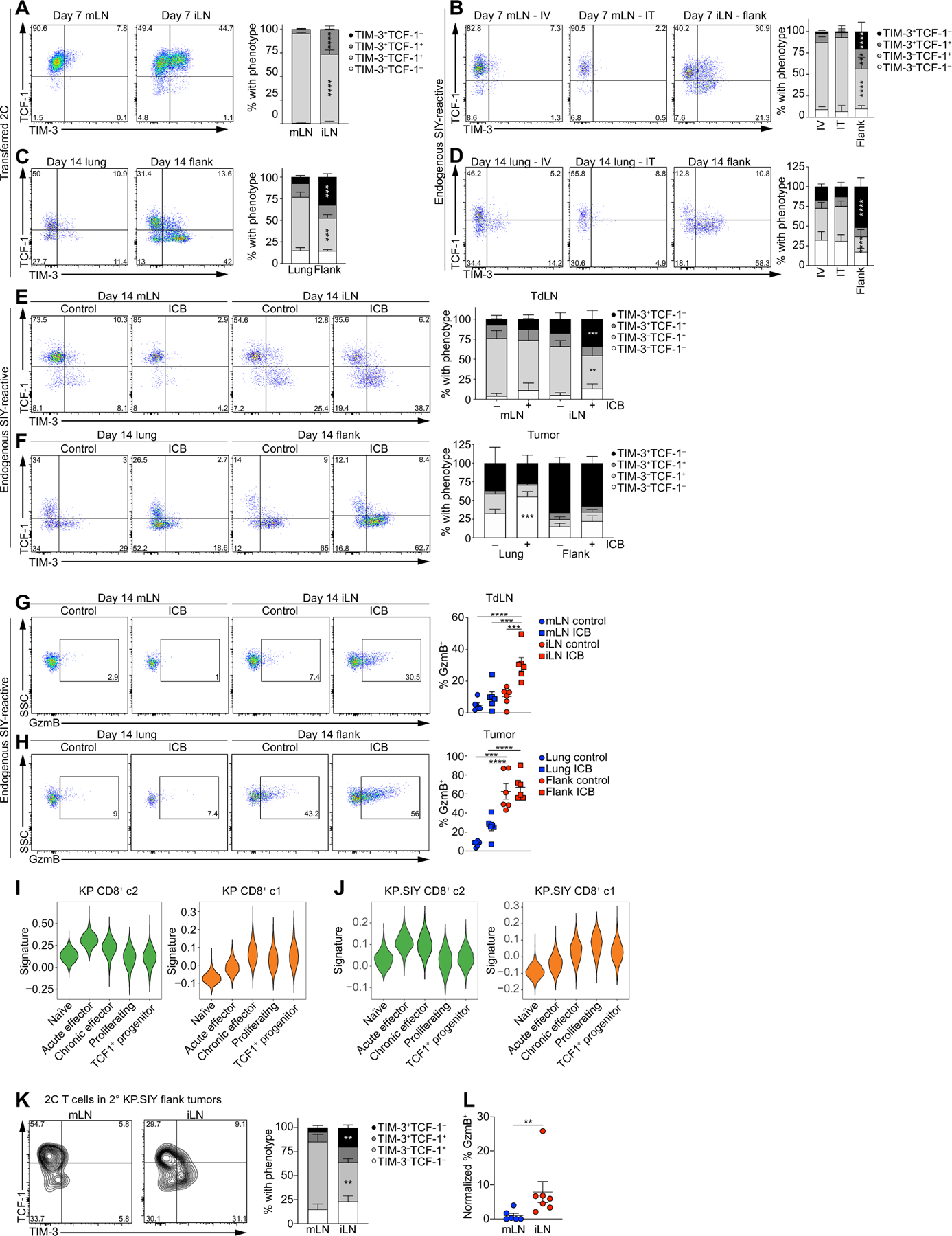
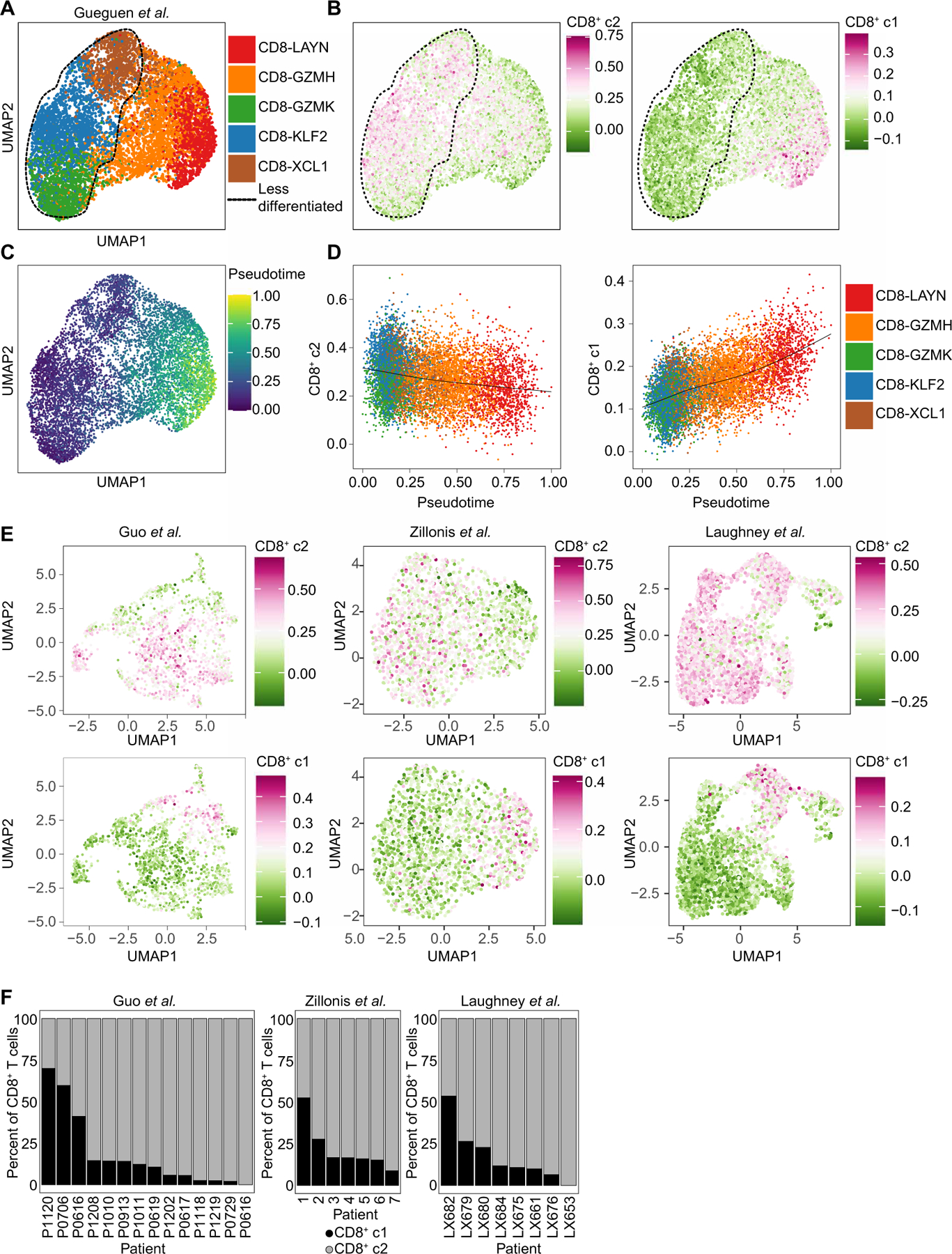
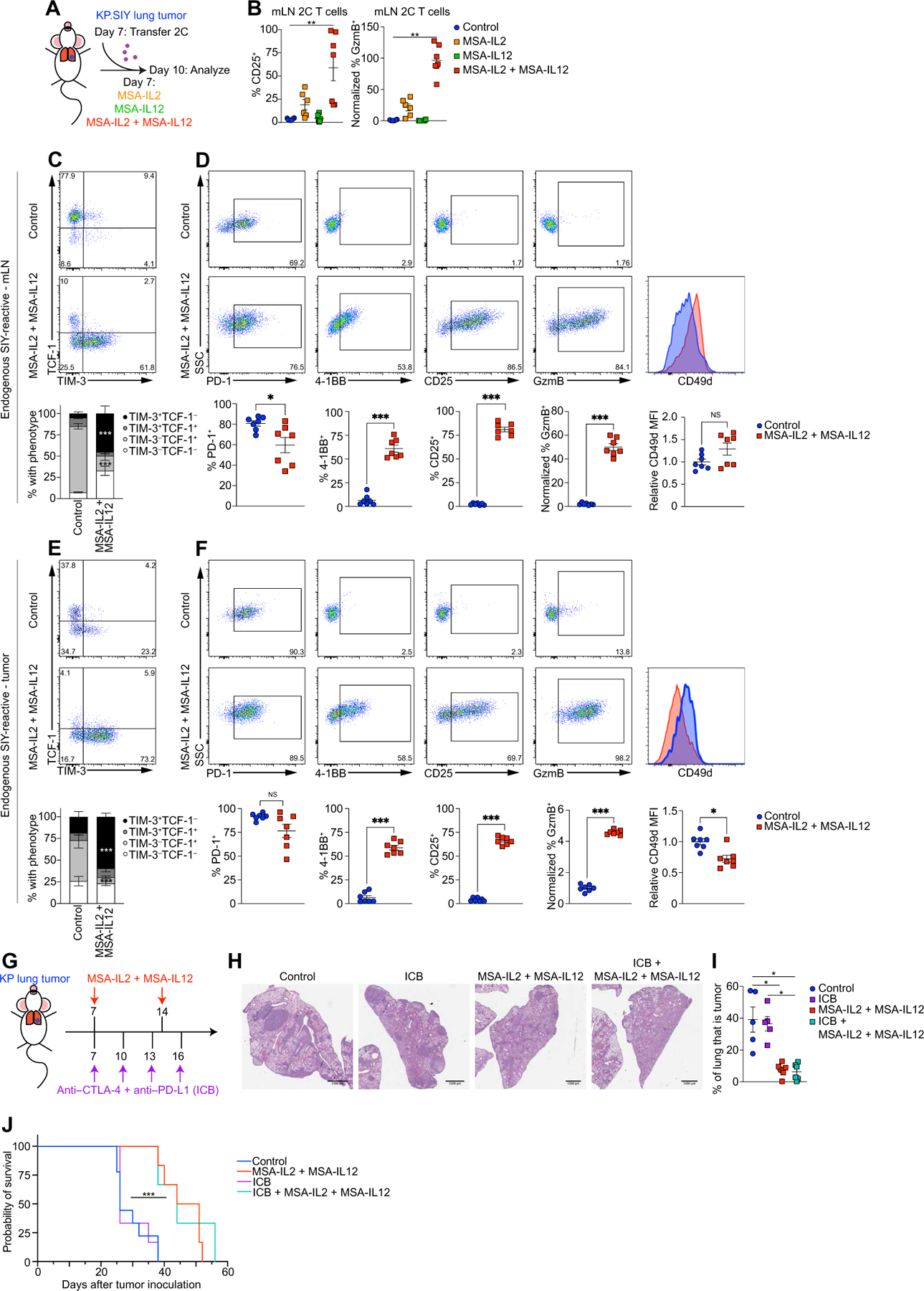
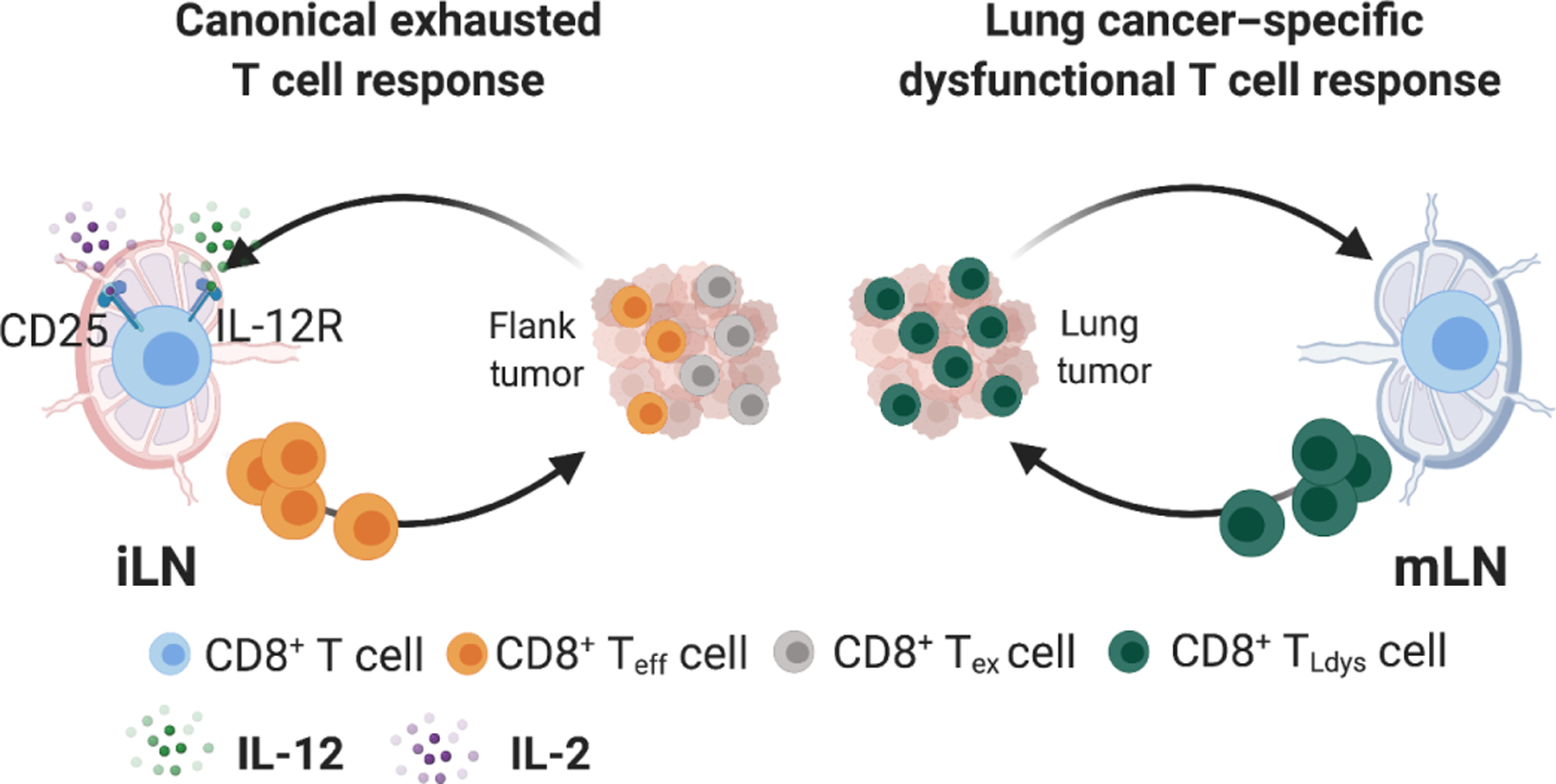
In non–small cell lung cancer (NSCLC), response to immune checkpoint blockade (ICB) is associated with programmed cell death ligand 1 expression that is induced by interferon-γ–producing, tumor-infiltrating CD8+ T cells. However, not all tumors with a CD8+ T cell infiltrate respond to ICB, and little is known about the mechanisms governing ICB resistance in T cell–infiltrated NSCLC. We used an orthotopic NSCLC mouse model to study ICB-refractory CD8+ T cell responses. Single-cell RNA sequencing of the NSCLC mouse tumors revealed that lung cancer–specific tumor-infiltrating CD8+ T cells exhibited clonal expansion but lacked expression of genes associated with effector and exhausted T cell responses, indicating that they underwent a differentiation program distinct from conventional T cell exhaustion. This lung cancer–specific T cell dysfunction program was established early during priming in the mediastinal lymph node and was characterized by robust proliferation but a failed up-regulation of effector and exhausted T cell characteristics. Intriguingly, CD8+ T cells from patients with NSCLC expressed an analogous gene expression program, which appeared distinct from conventional T cell exhaustion. Administration of recombinant interleukin-2 (IL-2) and IL-12 was sufficient to restore effector T cell differentiation and induce control of KP lung tumors. These findings imply that a CD8+ T cell differentiation trajectory, activated during T cell priming in the mediastinal lymph node, limits the response of CD8+ T cells to ICB and thereby may contribute to failure of ICB in a subset T cell–infiltrated NSCLC.
Conflict of interest statement
Figures
References
-
- Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, Horn L, Drake CG, Pardoll DM, Chen L, Sharfman WH, Anders RA, Taube JM, McMiller TL, Xu H, Korman AJ, Jure-Kunkel M, Agrawal S, McDonald D, Kollia GD, Gupta A, Wigginton JM, Sznol M, Safety, activity, and immune correlates of anti–PD-1 antibody in cancer. N. Engl. J. Med 366, 2443–2454 (2012). - PMC - PubMed
-
- Rafei H, El-Bahesh E, Finianos A, Nassereddine S, Tabbara I, Immune-based therapies for non-small cell lung cancer. Anticancer Res 37, 377–387 (2017). - PubMed
-
- Herbst RS, Soria JC, Kowanetz M, Fine GD, Hamid O, Gordon MS, Sosman JA, McDermott DF, Powderly JD, Gettinger SN, Kohrt HE, Horn L, Lawrence DP, Rost S, Leabman M, Xiao Y, Mokatrin A, Koeppen H, Hegde PS, Mellman I, Chen DS, Hodi FS, Predictive correlates of response to the anti–PD-L1 antibody MPDL3280A in cancer patients. Nature 515, 563–567 (2014). - PMC - PubMed
-
- Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, Park K, Smith D, Artal-Cortes A, Lewanski C, Braiteh F, Waterkamp D, He P, Zou W, Chen DS, Yi J, Sandler A, Rittmeyer A; POPLAR Study Group, Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016). - PubMed
-
- Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, Cowey CL, Schadendorf D, Wagstaff J, Dummer R, Ferrucci PF, Smylie M, Hogg D, Hill A, Marquez-Rodas I, Haanen J, Guidoboni M, Maio M, Schoffski P, Carlino MS, Lebbe C,McArthur G, Ascierto PA, Daniels GA, Long GV, Bastholt L, Rizzo JI, Balogh A, Moshyk A, Hodi FS, Wolchok JD, Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med 381, 1535–1546 (2019). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
