

Safety and immunogenicity of 2-dose heterologous Ad26.ZEBOV, MVA-BN-Filo Ebola vaccination in healthy and HIV-infected adults: A randomised, placebo-controlled Phase II clinical trial in Africa
- PMID: 34714820
- PMCID: PMC8555783
- DOI: 10.1371/journal.pmed.1003813
Safety and immunogenicity of 2-dose heterologous Ad26.ZEBOV, MVA-BN-Filo Ebola vaccination in healthy and HIV-infected adults: A randomised, placebo-controlled Phase II clinical trial in Africa
Abstract
Background: We investigated safety, tolerability, and immunogenicity of the heterologous 2-dose Ebola vaccination regimen in healthy and HIV-infected adults with different intervals between Ebola vaccinations.
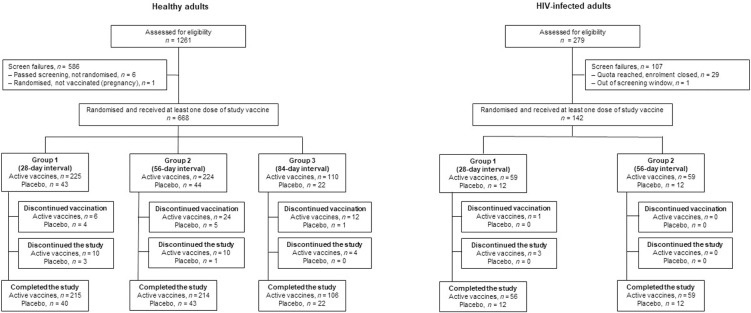
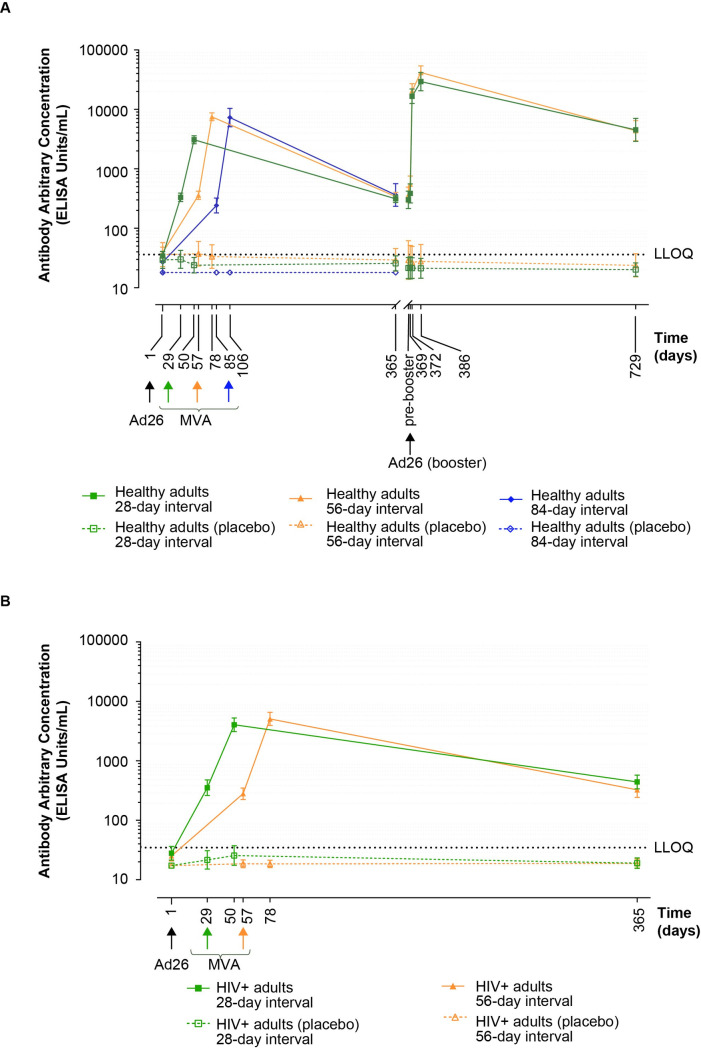
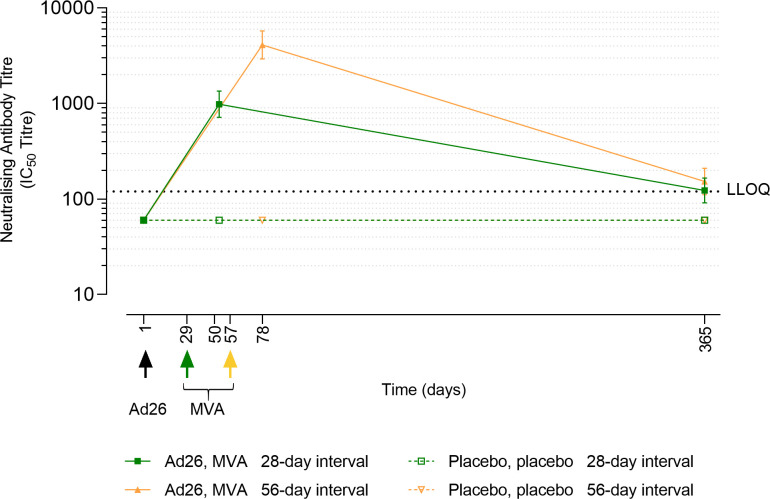
Methods and findings: In this randomised, observer-blind, placebo-controlled Phase II trial, 668 healthy 18- to 70-year-olds and 142 HIV-infected 18- to 50-year-olds were enrolled from 1 site in Kenya and 2 sites each in Burkina Faso, Cote d'Ivoire, and Uganda. Participants received intramuscular Ad26.ZEBOV followed by MVA-BN-Filo at 28-, 56-, or 84-day intervals, or saline. Females represented 31.4% of the healthy adult cohort in contrast to 69.7% of the HIV-infected cohort. A subset of healthy adults received booster vaccination with Ad26.ZEBOV or saline at Day 365. Following vaccinations, adverse events (AEs) were collected until 42 days post last vaccination and serious AEs (SAEs) were recorded from signing of the ICF until the end of the study. The primary endpoint was safety, and the secondary endpoint was immunogenicity. Anti-Ebola virus glycoprotein (EBOV GP) binding and neutralising antibodies were measured at baseline and at predefined time points throughout the study. The first participant was enrolled on 9 November 2015, and the date of last participant's last visit was 12 February 2019. No vaccine-related SAEs and mainly mild-to-moderate AEs were observed among the participants. The most frequent solicited AEs were injection-site pain (local), and fatigue, headache, and myalgia (systemic), respectively. Twenty-one days post-MVA-BN-Filo vaccination, geometric mean concentrations (GMCs) with 95% confidence intervals (CIs) of EBOV GP binding antibodies in healthy adults in 28-, 56-, and 84-day interval groups were 3,085 EU/mL (2,648 to 3,594), 7,518 EU/mL (6,468 to 8,740), and 7,300 EU/mL (5,116 to 10,417), respectively. In HIV-infected adults in 28- and 56-day interval groups, GMCs were 4,207 EU/mL (3,233 to 5,474) and 5,283 EU/mL (4,094 to 6,817), respectively. Antibody responses were observed until Day 365. Ad26.ZEBOV booster vaccination after 1 year induced an anamnestic response. Study limitations include that some healthy adult participants either did not receive dose 2 or received dose 2 outside of their protocol-defined interval and that the follow-up period was limited to 365 days for most participants.
Conclusions: Ad26.ZEBOV, MVA-BN-Filo vaccination was well tolerated and immunogenic in healthy and HIV-infected African adults. Increasing the interval between vaccinations from 28 to 56 days improved the magnitude of humoral immune responses. Antibody levels persisted to at least 1 year, and Ad26.ZEBOV booster vaccination demonstrated the presence of vaccination-induced immune memory. These data supported the approval by the European Union for prophylaxis against EBOV disease in adults and children ≥1 year of age.
Trial registration: ClinicalTrials.gov NCT02564523.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: HB, CB, LR reports grants from IMI2-2 [Grant Agreement EBOVAC2 (No.115861) from the Innovative Medicines Initiative 2 Joint Undertaking which receives support from the European Union’s Horizon 2020 research and innovation programme], during the conduct of the study. SBS reports grants from Janssen Vaccines and Prevention, during the conduct of the study. GS, CR, AG, DH, VB, KL, ML and MD were full-time employees of Janssen, Pharmaceutical Companies of Johnson & Johnson at the time of the study, and declared ownership of shares in Janssen, Pharmaceutical Companies of Johnson & Johnson. All other authors have nothing to disclose.
Figures
References
-
- World Health Organization. Situation Report: Ebola Virus Disease 10 June 2016. Available from: https://apps.who.int/iris/bitstream/handle/10665/208883/ebolasitrep_10Ju....
-
- World Health Organization. 10th Ebola outbreak in the Democratic Republic of the Congo declared over; vigilance against flare-ups and support for survivors must continue. [cited 2021 Sept 1]. Available from: https://www.who.int/news/item/25-06-2020-10th-ebola-outbreak-in-the-demo....
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
