

Mobile interventions targeting common mental disorders among pregnant and postpartum women: An equity-focused systematic review
- PMID: 34714882
- PMCID: PMC8555821
- DOI: 10.1371/journal.pone.0259474
Mobile interventions targeting common mental disorders among pregnant and postpartum women: An equity-focused systematic review
Abstract
Introduction: Pregnant and postpartum women face major psychological stressors that put them at higher risk of developing common mental disorders, such as depression and anxiety. Yet, their limited access to and uptake of traditional mental health care is inequitable, especially during the COVID-19 pandemic. Mobile interventions emerged as a potential solution to this discontinued healthcare access, but more knowledge is needed about their effectiveness and impact on health equity. This equity-focused systematic review examined the effectiveness and equity impact of mobile interventions targeting common mental disorders among pregnant and postpartum women.
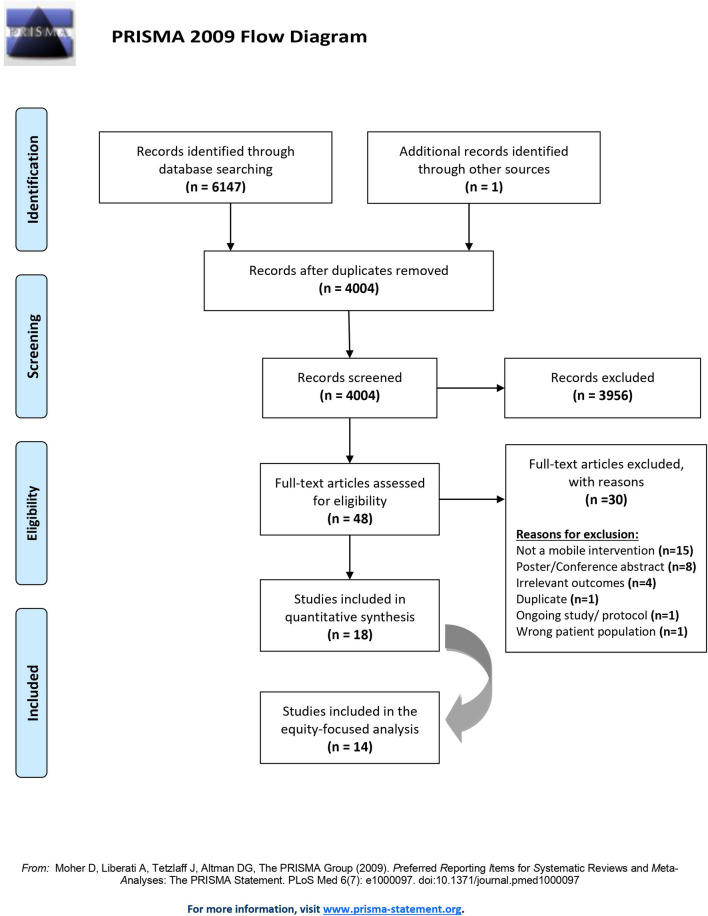
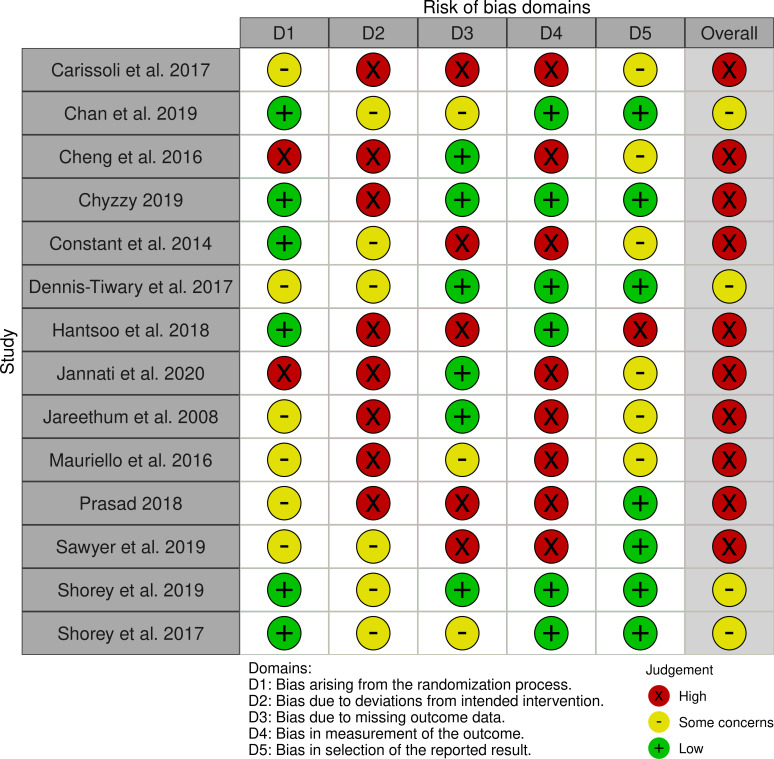
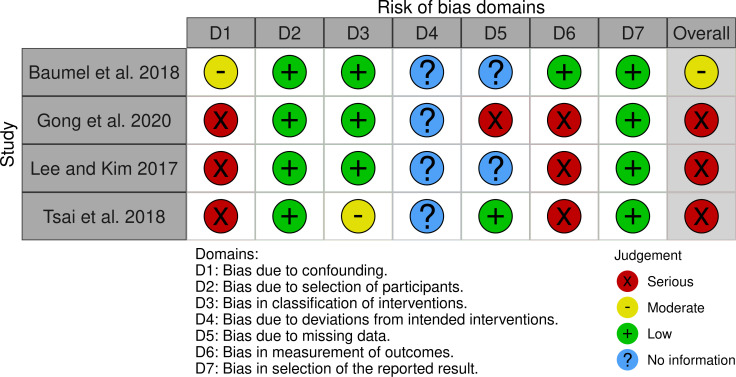
Methods and results: We systematically searched MEDLINE, EMBASE, PsychINFO and 3 other databases, from date of database inception and until January 2021, for experimental studies on mobile interventions targeting pregnant and postpartum women. We used pooled and narrative synthesis methods to analyze effectiveness and equity data, critically appraised the methodological rigour of included studies using Cochrane tools, and assessed the certainty of evidence using the GRADE approach. Our search identified 6148 records, of which 18 randomized and non-randomized controlled trials were included. Mobile interventions had a clinically important impact on reducing the occurrence of depression (OR = 0.51 [95% CI 0.41 to 0.64]; absolute risk reduction RD: 7.14% [95% CI 4.92 to 9.36]; p<0.001) and preventing its severity perinatally (MD = -3.07; 95% CI -4.68 to -1.46; p<0.001). Mobile cognitive behavioural therapy (CBT) was effective in managing postpartum depression (MD = -6.87; 95% CI -7.92 to -5.82; p<0.001), whereas other support-based interventions had no added benefit. Results on anxiety outcomes and utilization of care were limited. Our equity-focused analyses showed that ethnicity, age, education, and being primiparous were characteristics of influence to the effectiveness of mobile interventions.
Conclusion: As the COVID-19 pandemic has increased the need for virtual mental health care, mobile interventions show promise in preventing and managing common mental disorders among pregnant and postpartum women. Such interventions carry the potential to address health inequity but more rigorous research that examines patients' intersecting social identities is needed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Slade A, Cohen LJ, Sadler LS, et al.. The psychology and psychopathology of pregnancy. Handb Infant Ment Health 2009; 3: 22–39.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
