

Efficacy and safety of intermittent repeated levosimendan infusions in advanced heart failure patients: the LAICA study
- PMID: 34716753
- PMCID: PMC8712777
- DOI: 10.1002/ehf2.13670
Efficacy and safety of intermittent repeated levosimendan infusions in advanced heart failure patients: the LAICA study
Abstract
Aims: The aim of the LAICA study was to evaluate the long-term effectiveness and safety of intermittent levosimendan infusion in patients with advanced heart failure (AdHF).
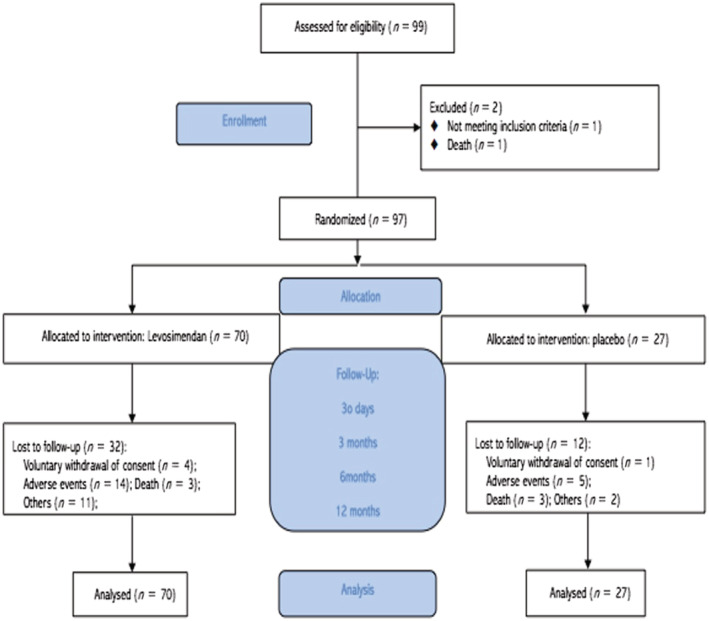
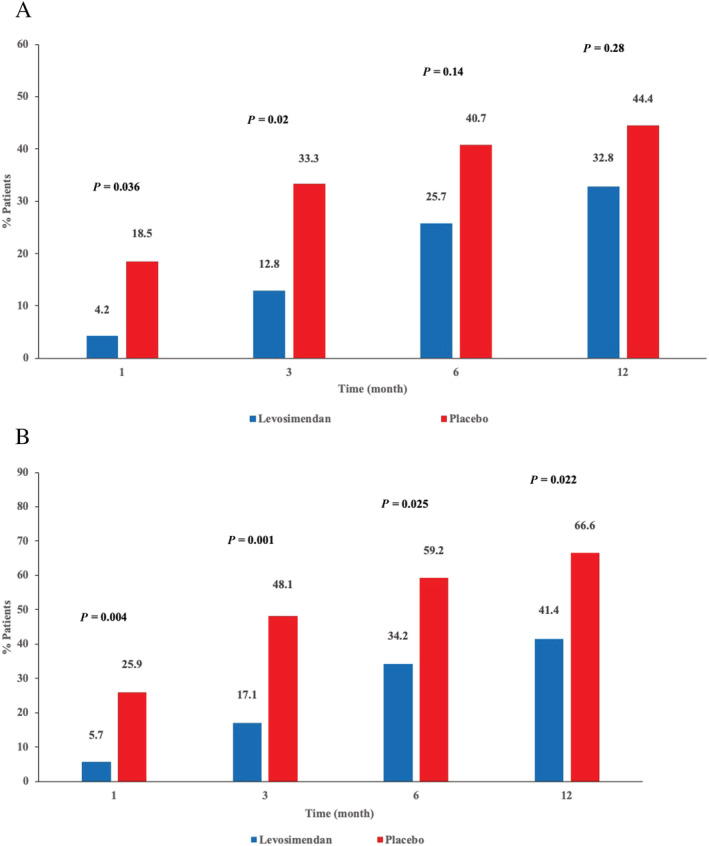
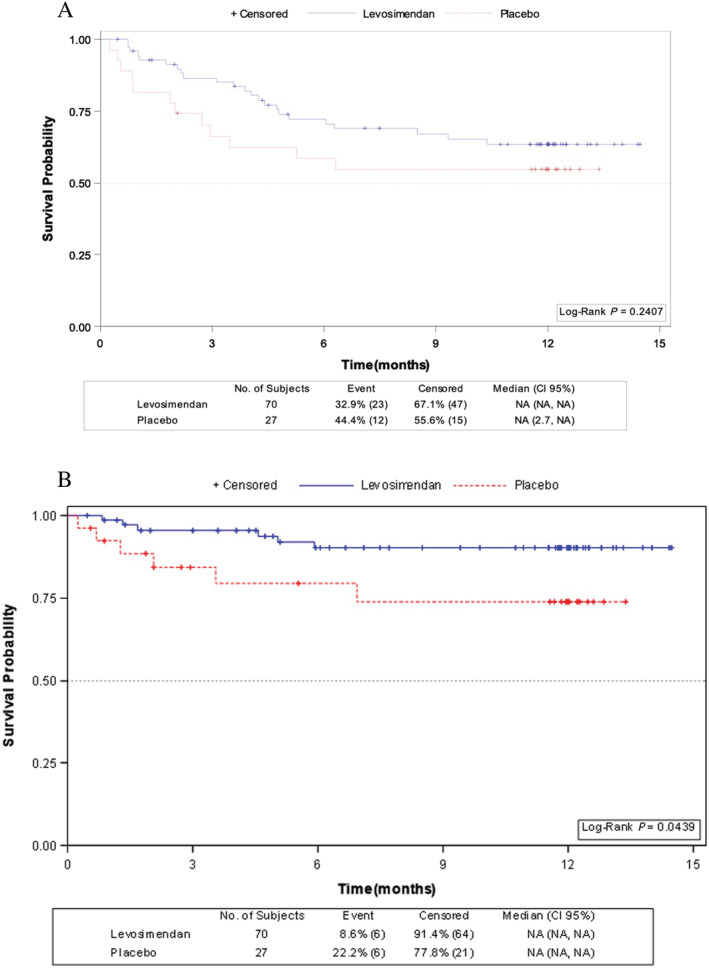
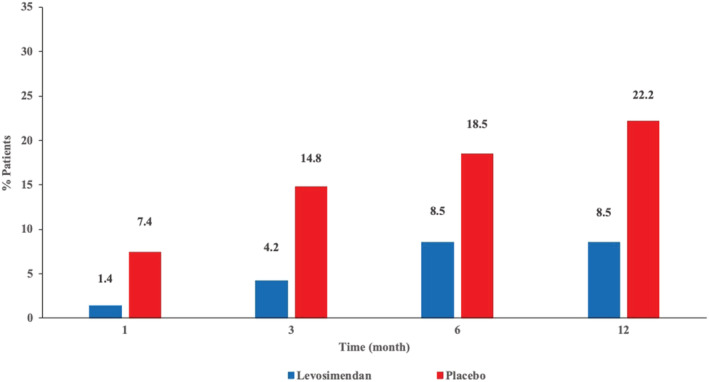
Methods and results: This was a multicentre, randomized, double-blind, placebo-controlled clinical trial of intermittent levosimendan 0.1 μg/kg/min as a continuous 24-h intravenous infusion administered once monthly for 1 year in patients with AdHF. The primary endpoint [incidence of rehospitalization (admission to the emergency department or hospital ward for >12 h) for acute decompensated HF or clinical deterioration of the underlying HF] occurred in 23/70 (33%) of the levosimendan group (Group I) and 12/27 (44%) of the placebo group (Group II) (P = 0.286). The incidence of hospital readmissions for acute decompensated HF (Group I vs. Group II) at 1, 3, 6, and 12 months was 4.2% vs. 18.2% (P = 0.036); 12.8% vs. 33.3% (P = 0.02); 25.7% vs. 40.7% (P = 0.147); 32.8% vs. 44.4% (P = 0.28), respectively. In a secondary pre-specified time-to-event analysis no differences were observed in admission for acute decompensated HF between patients treated with levosimendan compared with placebo (hazard ratio 0.66; 95% CI, 0.32-1.32; P = 0.24). Cumulative incidence for the aggregated endpoint of acute decompensation of HF and/or death at 1 and 3 months were significatively lower in the levosimendan group than in placebo group [5.7% vs. 25.9% (P = 0.004) and 17.1% vs. 48.1% (P = 0.001), respectively], but not at 6 and 12 months [34.2% vs. 59.2% (P = 0.025); 41.4% vs. 66.6% (P = 0.022), respectively]. Survival probability was significantly higher in patients who received levosimendan compared with those who received placebo (log rank: 4.06; P = 0.044). There were no clinically relevant differences in tolerability between levosimendan and placebo and no new safety signals were observed.
Conclusions: In our study, intermittent levosimendan in patients with AdHF produced a statistically non-significant reduction in the incidence of hospital readmissions for acute decompensated HF, a significantly lower cumulative incidence of acute decompensation of HF and/or death at 1 and 3 month of treatment and a significant improvement in survival during 12 months of treatment.
Keywords: Advanced heart failure; Inodilator; Intermittent administration; Levosimendan; Rehospitalization.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB, American Heart Association statistics committeestroke statistics subcommittee . Heart disease and stroke Statistics‐2016 update: American Heart Association statistics committee; stroke statistics subcommittee. Circulation 2016; 133: e38–e360. - PubMed
-
- Anguita Sánchez M, Crespo Leiro MG, De Teresa GE, Jiménez Navarro M, Alonso‐Pulpón L, Muñiz García J, PRICE study investigators . Prevalence of heart failure in the spanish general population aged over 45 years. the PRICE study. Rev Esp Cardiol 2008; 61: 1041–1049. - PubMed
-
- Stewart S, Jenkins A, Buchan S, McGuire A, Capewell S, McMurray JJ. The current cost of heart failure to the National Health Service in the UK. Eur J Heart Fail 2002; 4: 361–371. - PubMed
-
- McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez‐Sanchez MA, Jaarsma T, Kober L, Lip GYH, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Ronnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck‐Brentano C, Hasdai D, Hoes A, Kirchhof P, Knuuti J, Kolh P, McDonagh T, Moulin C, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, McDonagh T, Sechtem U, Bonet LA, Avraamides P, Ben Lamin HA, Brignole M, Coca A, Cowburn P, Dargie H, Elliott P, Flachskampf FA, Guida GF, Hardman S, Iung B, Merkely B, Mueller C, Nanas JN, Nielsen OW, Orn S, Parissis JT, Ponikowski P, ESC Committee for Practice Guidelines (CPG) , Document Reviewers . ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012; 14: 803–869. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
