

Effectiveness of an insurance enrollment support tool on insurance rates and cancer prevention in community health centers: a quasi-experimental study
- PMID: 34717616
- PMCID: PMC8557589
- DOI: 10.1186/s12913-021-07195-5
Effectiveness of an insurance enrollment support tool on insurance rates and cancer prevention in community health centers: a quasi-experimental study
Erratum in
-
Correction to: Effectiveness of an insurance enrollment support tool on insurance rates and cancer prevention in community health centers: a quasi-experimental study.BMC Health Serv Res. 2022 May 2;22(1):587. doi: 10.1186/s12913-022-07974-8. BMC Health Serv Res. 2022. PMID: 35501787 Free PMC article. No abstract available.
Abstract
Background: Following the ACA, millions of people gained Medicaid insurance. Most electronic health record (EHR) tools to date provide clinical-decision support and tracking of clinical biomarkers, we developed an EHR tool to support community health center (CHC) staff in assisting patients with health insurance enrollment documents and tracking insurance application steps. The objective of this study was to test the effectiveness of the health insurance support tool in (1) assisting uninsured patients gaining insurance coverage, (2) ensuring insurance continuity for patients with Medicaid insurance (preventing coverage gaps between visits); and (3) improving receipt of cancer preventive care.
Methods: In this quasi-experimental study, twenty-three clinics received the intervention (EHR-based insurance support tool) and were matched to 23 comparison clinics. CHCs were recruited from the OCHIN network. EHR data were linked to Medicaid enrollment data. The primary outcomes were rates of uninsured and Medicaid visits. The secondary outcomes were receipt of recommended breast, cervical, and colorectal cancer screenings. A comparative interrupted time-series using Poisson generalized estimated equation (GEE) modeling was performed to evaluate the effectiveness of the EHR-based tool on the primary and secondary outcomes.
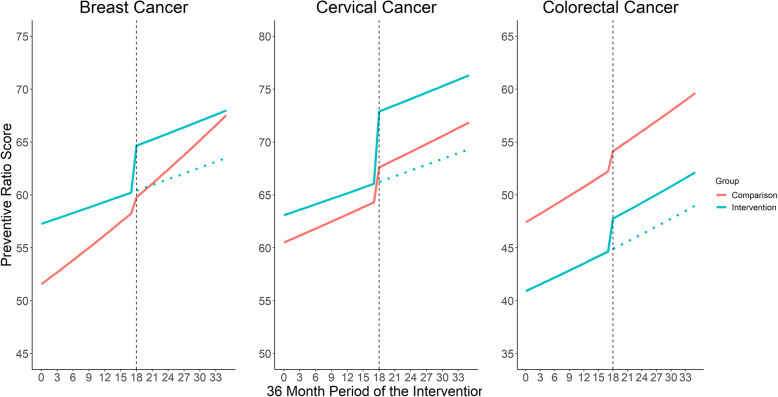
Results: Immediately following implementation of the enrollment tool, the uninsured visit rate decreased by 21.0% (Adjusted Rate Ratio [RR] = 0.790, 95% CI = 0.621-1.005, p = .055) while Medicaid-insured visits increased by 4.5% (ARR = 1.045, 95% CI = 1.013-1.079) in the intervention group relative to comparison group. Cervical cancer preventive ratio increased 5.0% (ARR = 1.050, 95% CI = 1.009-1.093) immediately following implementation of the enrollment tool in the intervention group relative to comparison group. Among patients with a tool use, 81% were enrolled in Medicaid 12 months after tool use. For the 19% who were never enrolled in Medicaid following tool use, most were uninsured (44%) at the time of tool use.
Conclusions: A health insurance support tool embedded within the EHR can effectively support clinic staff in assisting patients in maintaining their Medicaid coverage. Such tools may also have an indirect impact on evidence-based practice interventions, such as cancer screening.
Trial registration: This study was retrospectively registered on February 4th, 2015 with Clinicaltrials.gov (#NCT02355262). The registry record can be found at https://www.clinicaltrials.gov/ct2/show/NCT02355262 .
Keywords: Electronic health record tool; Health information technology; Health insurance; Implementation science; Medicaid; Navigator.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Key Facts about the Uninsured Population [https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-...].
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
