

New-onset versus relapsing giant cell arteritis treated with tocilizumab: 3-year results from a randomized controlled trial and extension
- PMID: 34718434
- PMCID: PMC9258533
- DOI: 10.1093/rheumatology/keab780
New-onset versus relapsing giant cell arteritis treated with tocilizumab: 3-year results from a randomized controlled trial and extension
Abstract
Objective: Tocilizumab plus prednisone induces sustained glucocorticoid-free remission in patients with GCA. However, its long-term benefits in new-onset vs relapsing disease are uncertain, and the value of weekly vs every-other-week dosing has not been evaluated.
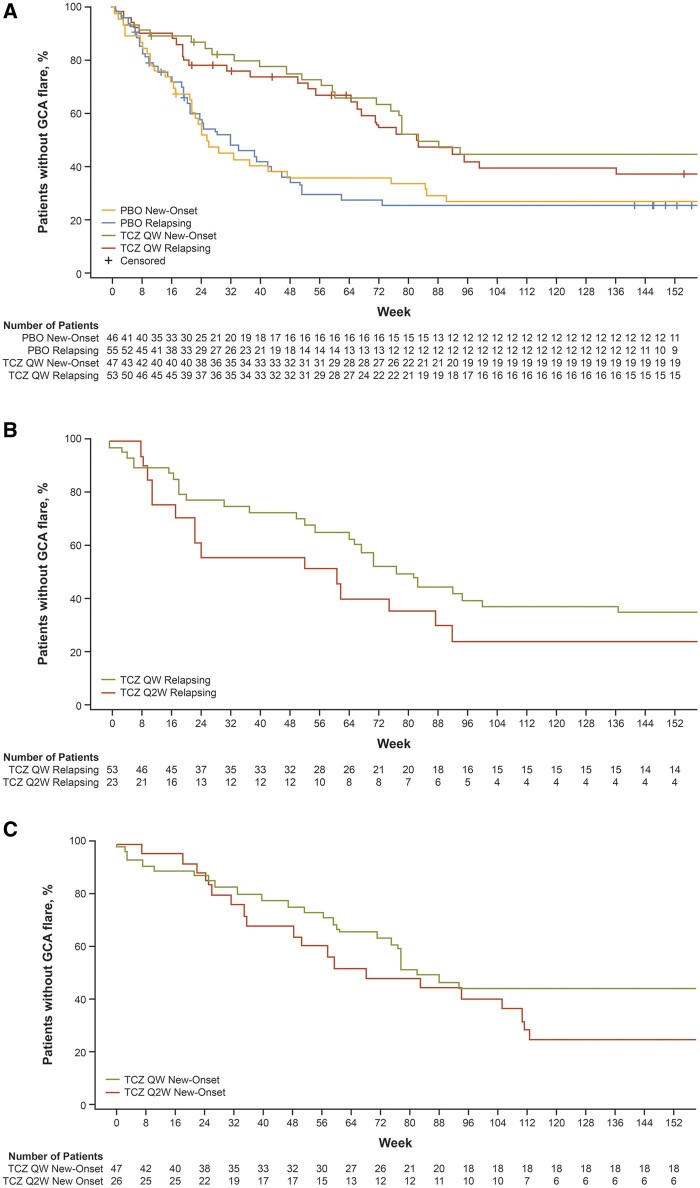
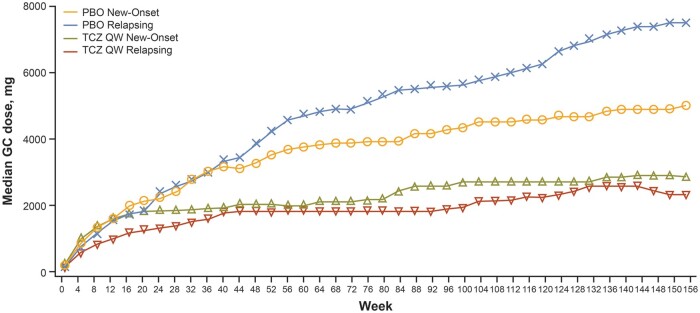
Methods: In Giant-Cell Arteritis Actemra (GiACTA) part 1, patients with new-onset or relapsing GCA received blinded tocilizumab weekly (TCZ QW), tocilizumab every-other-week (TCZ Q2W) or placebo for 52 weeks, with a prednisone taper. In part 2 (open-label), patients were treated at investigator discretion for 104 weeks. In this analysis, patients were evaluated according to their original treatment assignments, and outcomes beyond 52 weeks were assessed. Outcomes of interest included time to first flare and cumulative glucocorticoid exposure over 3 years according to baseline disease status.
Results: Part 1 enrolled 250 patients; 215 entered part 2. At baseline, 48% had new-onset disease and 52% had relapsing disease. In patients with new-onset and relapsing disease, the median time to first flare in the TCZ QW group was 577 and 575 days, respectively, vs 479 and 428 days with TCZ Q2W and 179 and 224 days with placebo; the median cumulative glucocorticoid dose was 3068 mg and 2191 mg with TCZ QW, 4080 mg and 2353 mg with TCZ Q2W, and 4639 mg and 6178 mg with placebo.
Conclusion: TCZ QW delayed the time to flare and reduced the cumulative glucocorticoid dose in patients with relapsing GCA and new-onset GCA. These data support initiating TCZ QW as part of first-line therapy in all patients with active GCA.
Trial registration: ClinicalTrials.gov, https://clinicaltrials.gov, NCT01791153.
Keywords: biologic therapies; cardiovascular; clinical trials and methods; giant cell arteritis; inflammation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
Comment in
-
Where do we go after GiACTA?Rheumatology (Oxford). 2022 Jul 6;61(7):2720-2721. doi: 10.1093/rheumatology/keac010. Rheumatology (Oxford). 2022. PMID: 35020808 No abstract available.
References
-
- Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B.. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology 2017;56:506–15. - PubMed
