

Progressive, Long-Term Hearing Loss in Congenital CMV Disease After Ganciclovir Therapy
- PMID: 34718680
- PMCID: PMC9590555
- DOI: 10.1093/jpids/piab095
Progressive, Long-Term Hearing Loss in Congenital CMV Disease After Ganciclovir Therapy
Abstract
Background: Long-term hearing outcomes among children with symptomatic congenital cytomegalovirus (CMV) disease who received 6-week ganciclovir therapy early in life are unknown.
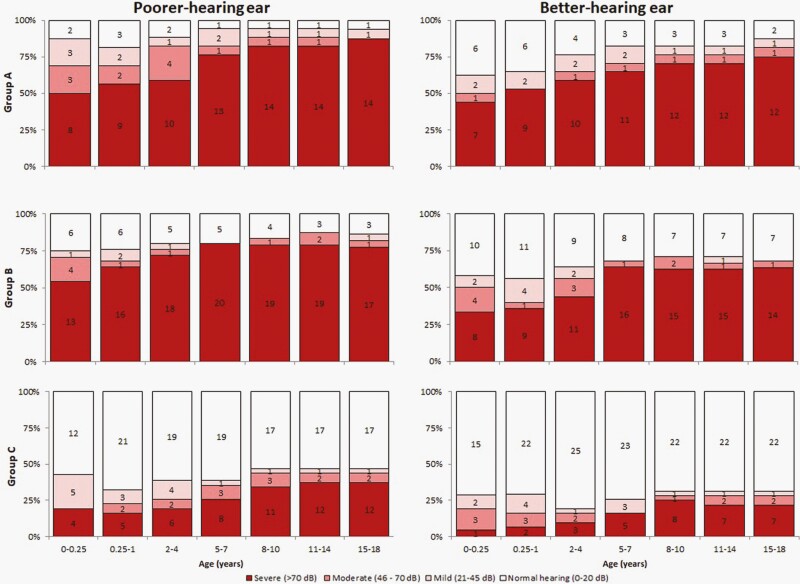
Methods: Longitudinal study of 76 children with symptomatic congenital CMV disease, born 1983-2005, who were categorized into three groups: group A treated with ganciclovir; group B untreated who had microcephaly, chorioretinitis, or sensorineural hearing loss (SNHL; ≥25 dB) diagnosed in the first month of life (congenital); and group C untreated who did not meet criteria for group B.
Results: Patients in groups A (n = 17), B (n = 27), and C (n = 32) were followed to median age of 13, 11, and 13 years, respectively. In group A, patients received ganciclovir for median of 40 (range, 11-63) days; 7 (41%) had grade 3 or 4 neutropenia. Congenital SNHL was diagnosed in 11 (65%) patients in group A, 15 (56%) in group B, and none in group C. Early-onset SNHL was diagnosed between ages ≥1-12 months in an additional 4 (24%), 6 (22%), and 8 (25%) patients in groups A, B, and C, respectively. By the end of follow-up, 12 (71%), 16 (59%), and 7 (22%) of patients in groups A, B, and C, respectively, had severe (>70 dB) SNHL in the better-hearing ear.
Conclusions: In this study, most patients with symptomatic congenital CMV disease and congenital or early-onset SNHL eventually developed hearing loss severe enough to have been potential candidates for cochlear implantation, with or without 6-week ganciclovir therapy. Understanding long-term hearing outcomes of patients treated with 6-month oral valganciclovir (current standard of care) is needed.
Keywords: congenital cytomegalovirus; ganciclovir; sensorineural hearing loss.
Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society 2021.
Figures
Comment in
-
Antiviral Therapy and Its Long-Term Impact on Hearing Loss Caused by Congenital Cytomegalovirus: Much Remains to Be Learned!J Pediatric Infect Dis Soc. 2022 May 30;11(5):186-189. doi: 10.1093/jpids/piab133. J Pediatric Infect Dis Soc. 2022. PMID: 35150282 No abstract available.
References
-
- Fowler KB, Ross SA, Shimamura M, et al. Racial and ethnic differences in the prevalence of congenital cytomegalovirus infection. J Pediatr 2018; 200:196–201.e1. - PubMed
-
- Dollard SC, Grosse SD, Ross DS. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev Med Virol 2007; 17:355–63. - PubMed
-
- Goderis J, De Leenheer E, Smets K, et al. Hearing loss and congenital CMV infection: a systematic review. Pediatrics 2014; 134:972–82. - PubMed
-
- Ahlfors K, Ivarsson SA, Harris S. Report on a long-term study of maternal and congenital cytomegalovirus infection in Sweden. Review of prospective studies available in the literature. Scand J Infect Dis 1999; 31:443–57. - PubMed
-
- Boppana SB, Fowler KB, Britt WJ, et al. Symptomatic congenital cytomegalovirus infection in infants born to mothers with preexisting immunity to cytomegalovirus. Pediatrics 1999; 104:55–60. - PubMed
