

Prevalence of BRAFV600 in glioma and use of BRAF Inhibitors in patients with BRAFV600 mutation-positive glioma: systematic review
- PMID: 34718782
- PMCID: PMC8972326
- DOI: 10.1093/neuonc/noab247
Prevalence of BRAFV600 in glioma and use of BRAF Inhibitors in patients with BRAFV600 mutation-positive glioma: systematic review
Abstract
Background: Detailed prevalence estimates of BRAFV600 mutations and BRAF inhibitor (BRAFi) treatment responses in V600-mutant glioma will inform trial development.
Methods: Our systematic review analyzed overall prevalence of BRAFV600 mutations in glioma and BRAFi treatment response.
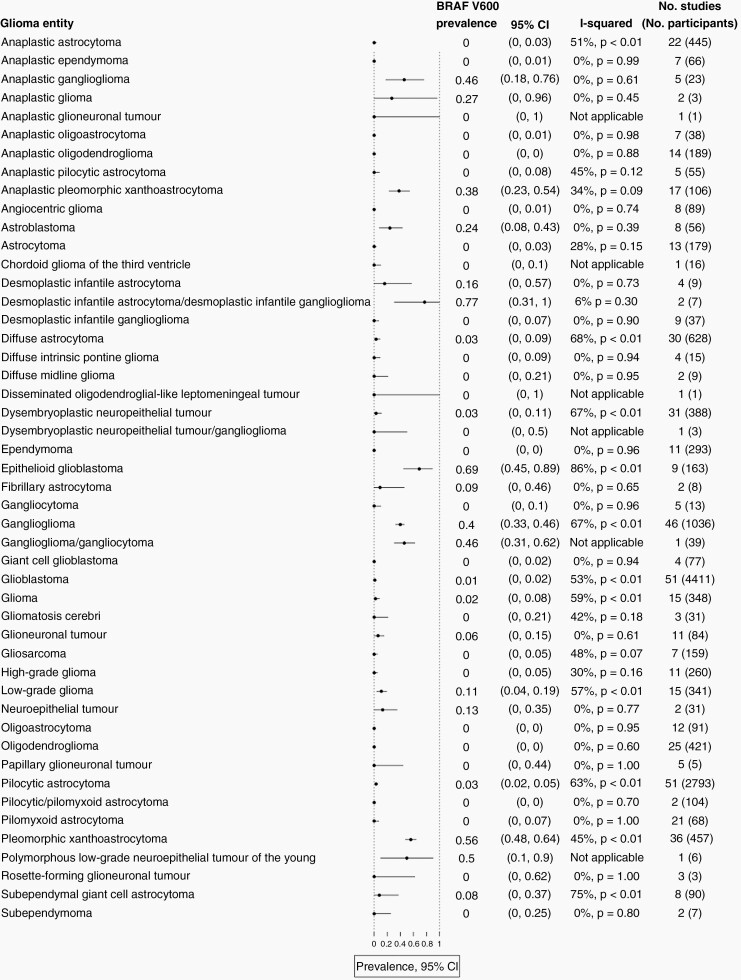
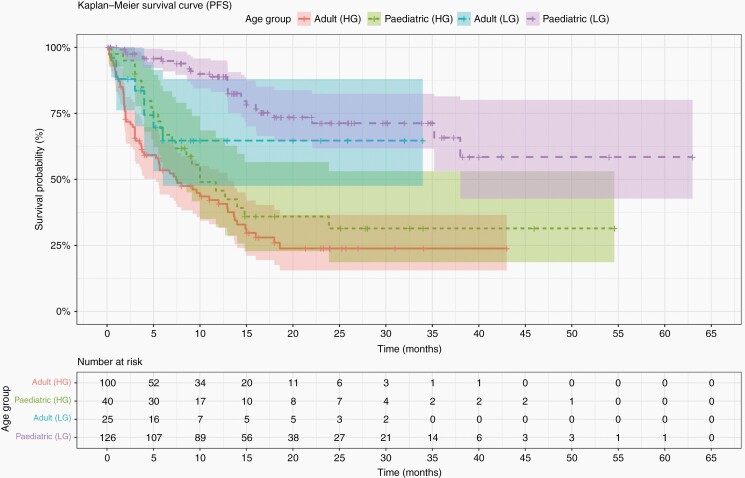
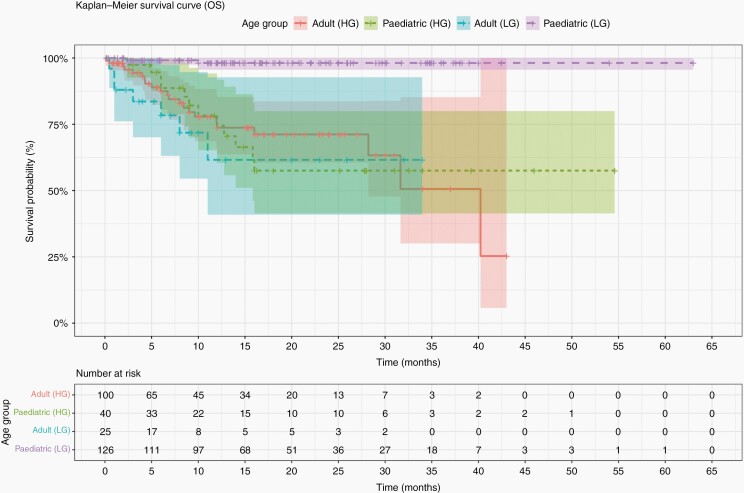
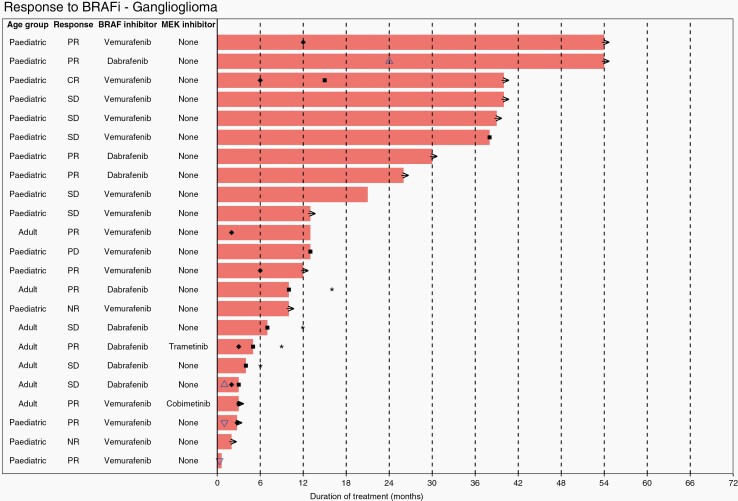
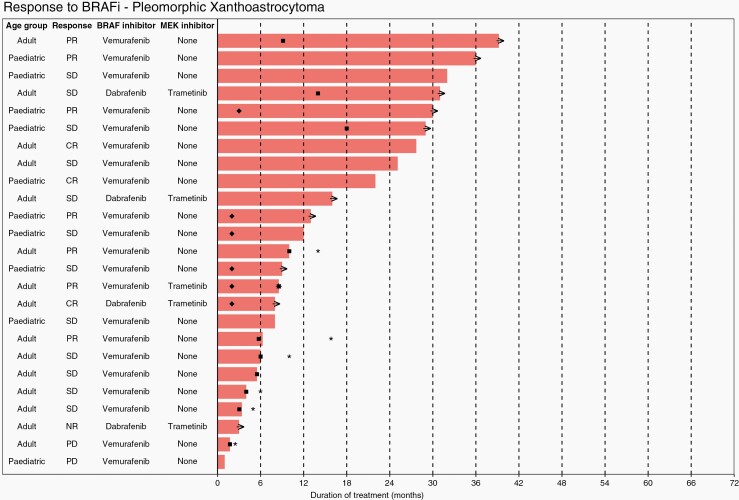
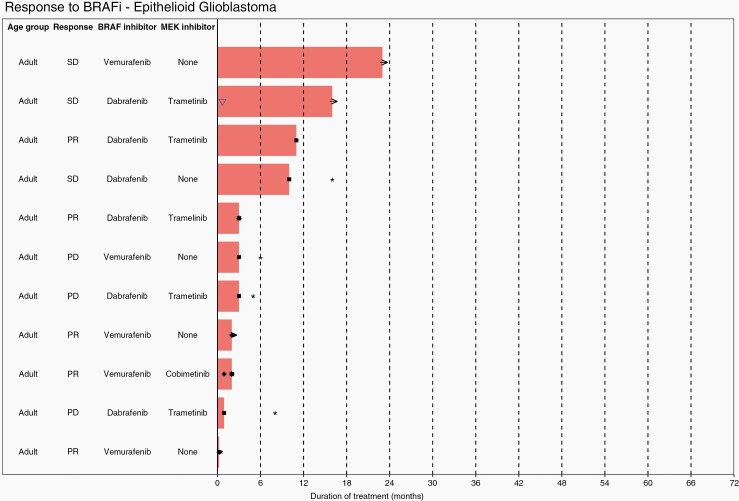
Results: Based on 13 682 patients in 182 publications, the prevalence of BRAFV600 in epithelioid glioblastoma (eGBM) was 69% [95% CI: 45-89%]; pleomorphic xanthoastrocytoma (PXA): 56% [48-64%] anaplastic pleomorphic xanthoastrocytoma (aPXA): 38% [23-54%], ganglioglioma (GG): 40% [33-46%], and anaplastic ganglioglioma (aGG): 46% [18-76%]. Prevalence in astroblastoma was 24% [8-43%], desmoplastic infantile astrocytoma (DIA): 16% [0-57%], subependymal giant cell astrocytoma (SEGA): 8% [0-37%], dysembryoplastic neuroepithelial tumor (DNET): 3% [0-11%], diffuse astrocytoma (DA): 3% [0-9%], and pilocytic astrocytoma (PA): 3% [2-5%]. We reviewed 394 V600-mutant gliomas treated with BRAFi from 130 publications. One hundred and twenty-nine pediatric low-grade gliomas showed 4 (3.1%) complete response (CR); 53 (41.1%) partial response (PR); 64 (49.6%) stable disease (SD) and 8 (6.2%) progressive disease (PD). 25 pediatric high-grade gliomas showed CR; PR; SD; PD in 4 (16.0%); 10 (40.0%), 4 (16.0%); and 7 (28.0%) respectively. Thirty-nine adult low-grade gliomas showed CR; PR; SD; PD of 4 (10.3%); 17 (43.6%); 16 (41.0%) and 2 (5.1%) respectively. Ninety-seven adult high-grade gliomas showed CR; PR; SD; PD of 6 (6.2%); 31 (32.0%); 27 (27.8%); and 33 (34.0%) respectively.
Conclusions: BRAFV600 prevalence is highest in eGBM, PXA, aPXA, GG, aGG, and lower in astroblastoma, DIA, SEGA, DNET, DA, and PA. Our data provide the rationale for adjuvant clinical trials of BRAFi in V600-mutant glioma.
Keywords: BRAF; BRAF inhibitors; glioma; prevalence; systematic review.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Dankner M, Rose AAN, Rajkumar S, Siegel PM, Watson IR. Classifying BRAF alterations in cancer: new rational therapeutic strategies for actionable mutations. Oncogene. 2018;37(24):3183–3199. - PubMed
-
- Malumbres M, Barbacid M. RAS oncogenes: the first 30 years. Nat Rev Cancer. 2003;3(6):459–465. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
