

Review
doi: 10.1016/j.jcot.2021.101610.
eCollection 2021 Nov.
Imaging update on cartilage
Affiliations
- PMID: 34722147
- PMCID: PMC8531853
- DOI: 10.1016/j.jcot.2021.101610
Item in Clipboard
Review
Imaging update on cartilage
J Clin Orthop Trauma.
.
Abstract
In this update article, we present a review of the literature regarding the physiology of the articular cartilage, role of MR imaging in cartilage assessment, MRI sequences and protocols for cartilage imaging, brief overview of classifications and nomenclature for chondral and osteochondral lesions, MR imaging following cartilage repair and degenerative osteoarthritis.
Keywords: Cartilage imaging; Cartilage repair; Chondromalacia; MRI; Osteochondral lesions.
© 2021 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
We hereby declare that we have no conflict of interest.
Figures

MR Sequences for evaluation of patellar cartilage (a) FS PDW axial image (b) Non-FS PDW axial image (c) 3D T2∗ GRE image showing normal patellar cartilage.

(a) PD non-FS axial image of patellar cartilage showing a full thickness chondral defect at lateral patellar cartilage. (b) T2 mapping of the patellar cartilage: increased T2 relaxation values (ranging from 5 to 60 ms) at the level of morphologically evident chondral defect (Zone B) as compared from T2 relaxation values (ranging from 31 to 41 ms) in adjacent normal appearing cartilage (zone A and C).
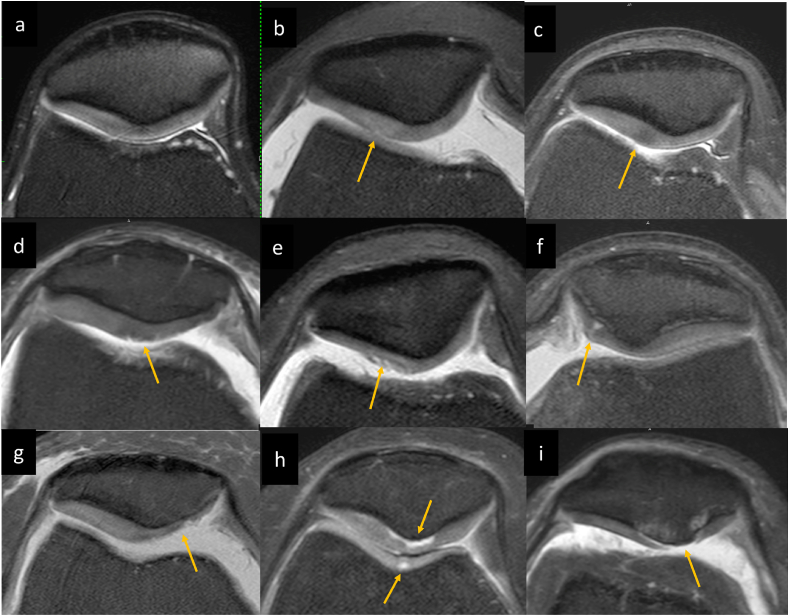
ICRS Grades of chondromalacia: (a) Normal patellar cartilage (b) Grade 1a intrinsic cartilage signal abnormality (hyperintense signal) without detectable morphologic changes (c) Grade 1a intrinsic cartilage signal abnormality (hypointense signal) without detectable morphologic changes (d) Grade 1b showing superficial fissures (e) Grade 2 focal chondral fissures involving <50% thickness of the cartilage. (f) Grade 3 focal cartilage fissure extending to > 50% of cartilage depth but not through the subchondral bone. (g) Grade 3 partial thickness cartilage loss >50% cartilage thickness without subchondral marrow changes in degenerative knee. (h) Chondral delamination is also included in grade 3 which are detected as fluid signal intensity subjacent to cortex without subchondral marrow changes, noted in patellar apex as well as trochlea in this case. (I) Grade 4 full thickness chondral lesions with subchondral marrow changes.

PD FS sagittal in a 48-year-old female shows a linear low signal in lateral femoral cartilage, perpendicular to the subchondral bone on T2 weighted images, located in morphologically normal appearing cartilage suggest” cartilage black line” sign. (b, c) PD FS images of another 54-year-old female with focal T2 hypointense chondral signal involving patellar cartilage with smooth overlying chondral surface could represent early chondral degeneration.

Grade 3 chondral lesion: (a, b) Consecutive T2W FS coronal images (c) PD FS sagittal image shows a full thickness chondral fissure extending posteriorly parallel to the subchondral bone to form a chondral flap at weight bearing aspect of medial femoral condyle without subchondral marrow edema.

Post microfracture MR imaging (a, b) PD FS sagittal and coronal images of a 49-year-old male presenting with knee pain and instability following a fall 2 years ago shows a full thickness chondral loss with subchondral cystic changes and marrow edema at posterior weight bearing aspect of medial femoral condyle. Note grade III longitudinal tear at peripheral aspect of posterior horn of medial meniscus evident on sagittal images. He also had complete ACL tear (not shown in images) (c,d) 1.5 year follow up MR imaging following microfracture and ACL reconstruction shows re-growth of cartilage with near complete filling of previously noted full thickness chondral loss at posterior weight bearing aspect of medial femoral condyle and near complete resolution of subchondral marrow edema (at site of microfracture).
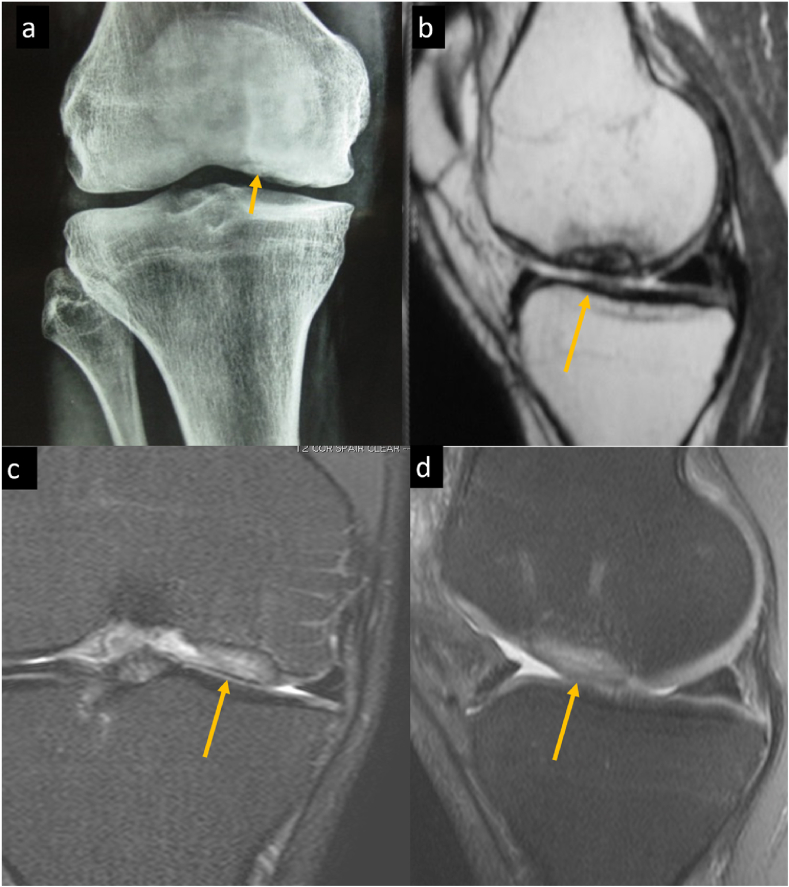
Post Cartilage repair MR imaging: 19-years-old male presenting with knee pain (a) AP radiograph of knee joint showing osteochondral lesion at weight bearing aspect of medial femoral condyle. (b) Sagittal non-FS PDW MR images shows a Stage 3 osteochondritis dissecans with undisplaced completely separated osteochondral fragment. (c) Coronal FS-PDW and (d) Sagittal FS-PDW MR images obtained 2.5 year following Autologous Chondrocyte implantation show complete integration of the chondral graft with the native cartilage and subchondral bone. Mildly proud chondral graft is noted with homogenous mildly hyperintense signal and subtle subchondral marrow edema-like signal that is not of much concern. Case Courtesy: Dr.Kalpesh Trivedi. Arthroscopy surgeon. Ahmedabad.

Schematic presentation of magnetic resonance imaging-based adaptation of the ICRS (International Cartilage Repair Society) staging system of osteochondritis dissecans (OCD) (a) Stable lesion in continuity with the host bone and covered by an intact articular cartilage is categorized as stage 1 OCD. (b) Stable lesion showing partial discontinuity of the cartilage from the host bone is categorized as stage 2 OCD. (c) Stage 3 OCD is characterized when there is an unstable lesion showing a complete discontinuity of the “dead in situ” lesion without dislodgement of the osteochondral fragment. (d) Stage 4 OCD is characterized by the presence of an osteochondral defect with a dislocated fragment.
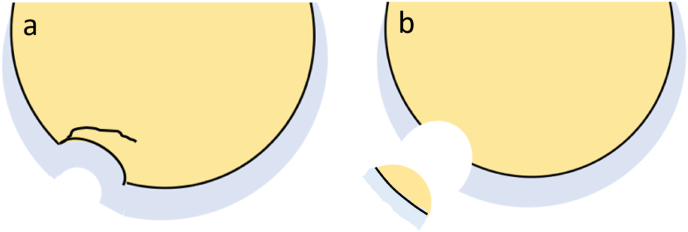
Schematic Presentation of Types of Osteochondral Fractures. (a) In the setting of an acute trauma, osteochondral fracture may present as an osteochondral lesion with a complete or incomplete fracture line through the articular cartilage and the sub-chondral bone with or without subchondral plate depression (b) The osteochondral fracture can also present as a localized defect involving the cartilage and the subchondral bone with a displaced osteochondral fracture fragment.

Osteochondral fracture (a, b) PD FS and non FS sagittal images of a 21-year-old male with history of twisting injury. These show an osteochondral fracture as evident by an incomplete fracture line at posterior (not shown in mages) aspect of lateral tibial plateau with adjacent marrow edema and subtle depression. He had associated ACL tear (Not shown in images). (c, d) PD FS axial and sagittal image of a 23-year-old male showing an osteochondral fracture at medial patellar facet with a displaced osteochondral fracture fragment at anterior aspect of knee joint in a case of transient patellar dislocation. Note bone marrow contusion at typical location at anterolateral aspect of lateral femoral condyle in (c).

ICRS Grades of osteochondritis Dessicans (OCD) (a, b) Stable lesion in continuity with the host bone and covered by an intact articular cartilage suggest Stage 1 OCD (c, d) Stable lesion showing partial discontinuity of the cartilage from the host bone (as marked by arrow) suggest Stage 2 OCD (e, f) Unstable lesion showing a complete discontinuity of the "dead in situ" lesion without dislocation of the fragment suggest Stage 3 OCD. (g, h) Presence of an osteochondral defect with a dislocated fragment suggest Stage 4 OCD.

Degenerative osteoarthritic changes (a) T2 weighted coronal and (b) PD weighted axial fat suppressed image of a 72 year old male with knee pain. (a) Shows diffuse full thickness chondral loss involving the weight bearing aspect of medial femoral and tibial plateau and (b) patellar apex with subchondral marrow edema. Superficial chondral surface defect is also noted in medial trochlea in (b). Marginal osteophytes are noted along femoral condyles in (a). These findings suggest degenerative osteoarthritic changes. Note subtle degenerative fraying of the free edge of body of medial meniscus without significant tear in (a).
References
-
- Buckwalter J.A., Hunzinker E., Rosenberg L. In: Injury and Repair of the Musculoskeletal Soft Tissues. Park Ridge, IL: American Academy of Orthopaedic Surgeons. Woo S.L.Y., Buckwalter J.A., editors. 1988. Articular cartilage: composition and structure; pp. 405–425.
-
- Buckwalter J.A., Mankin H.J. Articular cartilage, part 1: tissue design and chondrocyte-matrix interaction. J Bone Joint Surg Am. 1997;79:600–611.
-
- Newman A. Articular cartilage repair. Am J Sports Med. 1998;26:309–324. [PubMed: 9548130] - PubMed
-
- Patil Anupama, Jadhav Aniket. Imaging for cartilage injuries. Asian Journal of Arthroscopy. 2019 Jan - Apr;4(1):4–8.
Publication types
LinkOut - more resources
Full Text Sources