

Defining Factors Associated with High-quality Surgery Following Radical Cystectomy: Analysis of the British Association of Urological Surgeons Cystectomy Audit
- PMID: 34723215
- PMCID: PMC8546928
- DOI: 10.1016/j.euros.2021.08.005
Defining Factors Associated with High-quality Surgery Following Radical Cystectomy: Analysis of the British Association of Urological Surgeons Cystectomy Audit
Abstract
Background: Radical cystectomy (RC) is associated with high morbidity.
Objective: To evaluate healthcare and surgical factors associated with high-quality RC surgery.
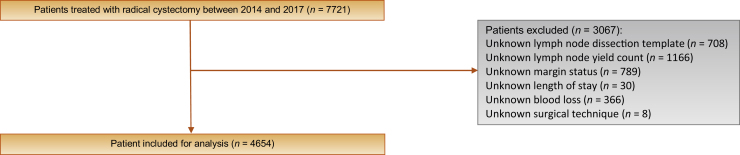
Design setting and participants: Patients within the prospective British Association of Urological Surgeons (BAUS) registry between 2014 and 2017 were included in this study.
Outcome measurements and statistical analysis: High-quality surgery was defined using pathological (absence of positive surgical margins and a minimum of a level I lymph node dissection template with a minimum yield of ten or more lymph nodes), recovery (length of stay ≤10 d), and technical (intraoperative blood loss <500 ml for open and <300 ml for minimally invasive RC) variables. A multilevel hierarchical mixed-effect logistic regression model was utilised to determine the factors associated with the receipt of high-quality surgery and index admission mortality.
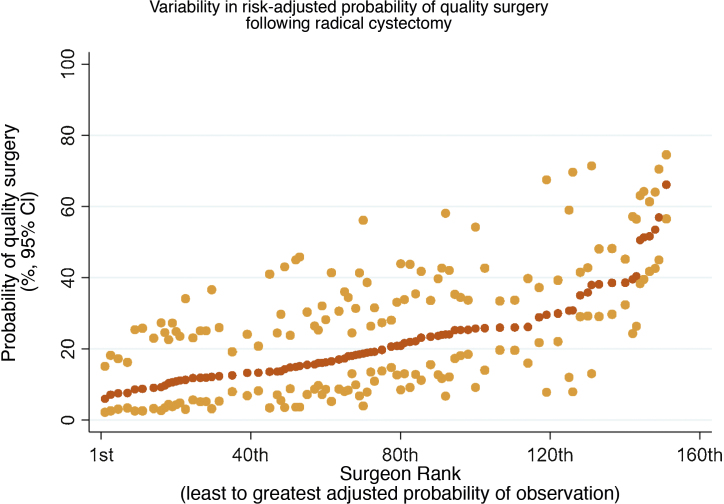
Results and limitations: A total of 4654 patients with a median age of 70.0 yr underwent RC by 152 surgeons at 78 UK hospitals. The median surgeon and hospital operating volumes were 23.0 and 47.0 cases, respectively. A total of 914 patients (19.6%) received high-quality surgery. The minimum annual surgeon volume and hospital volume of ≥20 RCs/surgeon/yr and ≥68 RCs/hospital/yr, respectively, were the thresholds determined to achieve better rates of high-quality RC. The mixed-effect logistic regression model found that recent surgery (odds ratio [OR]: 1.22, 95% confidence interval [CI]: 1.11-1.34, p < 0.001), laparoscopic/robotic RC (OR: 1.85, 95% CI: 1.45-2.37, p < 0.001), and higher annual surgeon operating volume (23.1-33.0 cases [OR: 1.54, 95% CI: 1.16-2.05, p = 0.003]; ≥33.1 cases [OR: 1.64, 95% CI: 1.18-2.29, p = 0.003]) were independently associated with high-quality surgery. High-quality surgery was an independent predictor of lower index admission mortality (OR: 0.38, 95% CI: 0.16-0.87, p = 0.021).
Conclusions: We report that annual surgeon operating volume and use of minimally invasive RC were predictors of high-quality surgery. Patients receiving high-quality surgery were independently associated with lower index admission mortality. Our results support the role of centralisation of complex oncology and implementation of a quality assurance programme to improve the delivery of care.
Patient summary: In this registry study of patients treated with surgical excision of the urinary bladder for bladder cancer, we report that patients treated by a surgeon with a higher annual operative volume and a minimally invasive approach were associated with the receipt of high-quality surgery. Patients treated with high-quality surgery were more likely to be discharged alive following surgery.
Keywords: Bladder cancer; British Association of Urological Surgeons audit; Centralisation; Outcomes; Quality surgery; Radical cystectomy.
© 2021 The Author(s).
Figures
Similar articles
-
The British Association of Urological Surgeons (BAUS) radical prostatectomy audit 2014/2015 - an update on current practice and outcomes by centre and surgeon case-volume.BJU Int. 2018 Jun;121(6):886-892. doi: 10.1111/bju.14156. Epub 2018 Feb 26. BJU Int. 2018. PMID: 29388311
-
Centralisation of radical cystectomies for bladder cancer in England, a decade on from the 'Improving Outcomes Guidance': the case for super centralisation.BJU Int. 2018 Feb;121(2):217-224. doi: 10.1111/bju.13929. Epub 2017 Jul 10. BJU Int. 2018. PMID: 28594471
-
Open radical cystectomy in England: the current standard of care - an analysis of the British Association of Urological Surgeons (BAUS) cystectomy audit and Hospital Episodes Statistics (HES) data.BJU Int. 2018 Jun;121(6):880-885. doi: 10.1111/bju.14143. Epub 2018 Feb 16. BJU Int. 2018. PMID: 29359882
-
The Importance of Hospital and Surgeon Volume as Major Determinants of Morbidity and Mortality After Radical Cystectomy for Bladder Cancer: A Systematic Review and Recommendations by the European Association of Urology Muscle-invasive and Metastatic Bladder Cancer Guideline Panel.Eur Urol Oncol. 2020 Apr;3(2):131-144. doi: 10.1016/j.euo.2019.11.005. Epub 2019 Dec 19. Eur Urol Oncol. 2020. PMID: 31866215
-
Optimizing surgical outcomes in bladder cancer patients undergoing radical cystectomy.Front Surg. 2023 Mar 14;9:1008318. doi: 10.3389/fsurg.2022.1008318. eCollection 2022. Front Surg. 2023. PMID: 36998470 Free PMC article. Review.
Cited by
-
Radical cystectomy and urinary diversion in women.Transl Androl Urol. 2023 Feb 28;12(2):155-157. doi: 10.21037/tau-23-4. Epub 2023 Feb 13. Transl Androl Urol. 2023. PMID: 36915872 Free PMC article. No abstract available.
-
Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial.JAMA. 2022 Jun 7;327(21):2092-2103. doi: 10.1001/jama.2022.7393. JAMA. 2022. PMID: 35569079 Free PMC article. Clinical Trial.
References
-
- Witjes J.A., Bruins H.M., Cathomas R. European Association of Urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol. 2021;79:82–104. - PubMed
-
- Tan W.S., Rodney S., Lamb B., Feneley M., Kelly J. Management of non-muscle invasive bladder cancer: A comprehensive analysis of guidelines from the United States, Europe and Asia. Cancer Treat Rev. 2016;47:22–31. - PubMed
-
- Goossens‐Laan C.A., Leliveld A.M., Verhoeven R.H. Effects of age and comorbidity on treatment and survival of patients with muscle‐invasive bladder cancer. Int J Cancer. 2014;135:905–912. - PubMed
-
- Shabsigh A., Korets R., Vora K.C. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur Urol. 2009;55:164–176. - PubMed
LinkOut - more resources
Full Text Sources
