

Contrastive learning improves critical event prediction in COVID-19 patients
- PMID: 34723227
- PMCID: PMC8542449
- DOI: 10.1016/j.patter.2021.100389
Contrastive learning improves critical event prediction in COVID-19 patients
Abstract
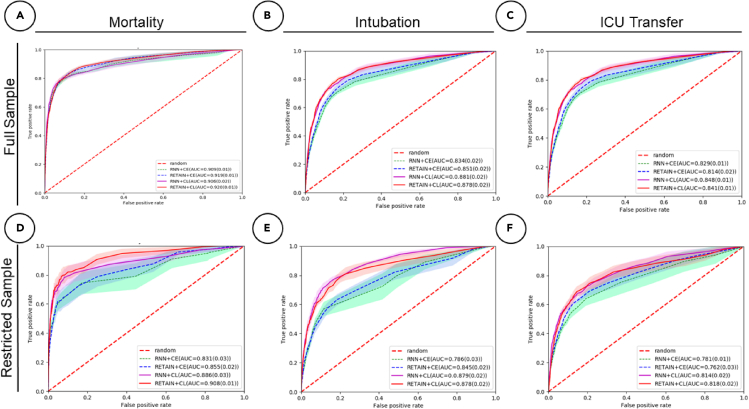
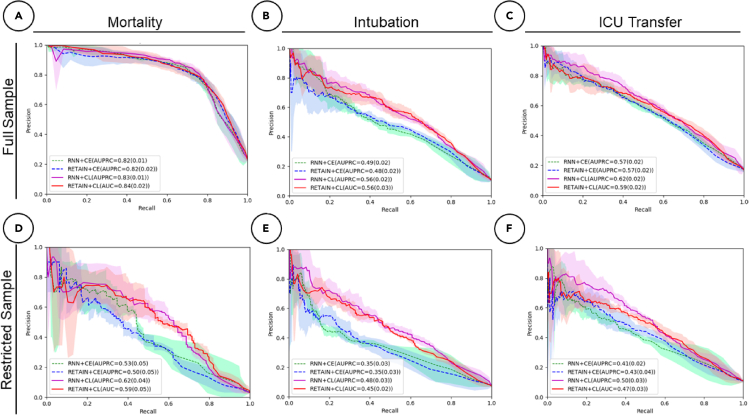
Deep learning (DL) models typically require large-scale, balanced training data to be robust, generalizable, and effective in the context of healthcare. This has been a major issue for developing DL models for the coronavirus disease 2019 (COVID-19) pandemic, where data are highly class imbalanced. Conventional approaches in DL use cross-entropy loss (CEL), which often suffers from poor margin classification. We show that contrastive loss (CL) improves the performance of CEL, especially in imbalanced electronic health records (EHR) data for COVID-19 analyses. We use a diverse EHR dataset to predict three outcomes: mortality, intubation, and intensive care unit (ICU) transfer in hospitalized COVID-19 patients over multiple time windows. To compare the performance of CEL and CL, models are tested on the full dataset and a restricted dataset. CL models consistently outperform CEL models, with differences ranging from 0.04 to 0.15 for area under the precision and recall curve (AUPRC) and 0.05 to 0.1 for area under the receiver-operating characteristic curve (AUROC).
Keywords: COVID-19; contrastive loss; deep learning; electronic health records; machine learning; recurrent neural network.
© 2021 The Authors.
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Contrastive Learning Improves Critical Event Prediction in COVID-19 Patients.ArXiv [Preprint]. 2021 Jan 11:arXiv:2101.04013v1. ArXiv. 2021. Update in: Patterns (N Y). 2021 Dec 10;2(12):100389. doi: 10.1016/j.patter.2021.100389. PMID: 33442560 Free PMC article. Updated. Preprint.
References
-
- Glicksberg B.S., Johnson K.W., Dudley J.T. The next generation of precision medicine: observational studies, electronic health records, biobanks and continuous monitoring. Hum. Mol. Genet. 2018;27:R56–R62. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
