

Polycystic Liver Disease: Advances in Understanding and Treatment
- PMID: 34724412
- PMCID: PMC8842879
- DOI: 10.1146/annurev-pathol-042320-121247
Polycystic Liver Disease: Advances in Understanding and Treatment
Abstract
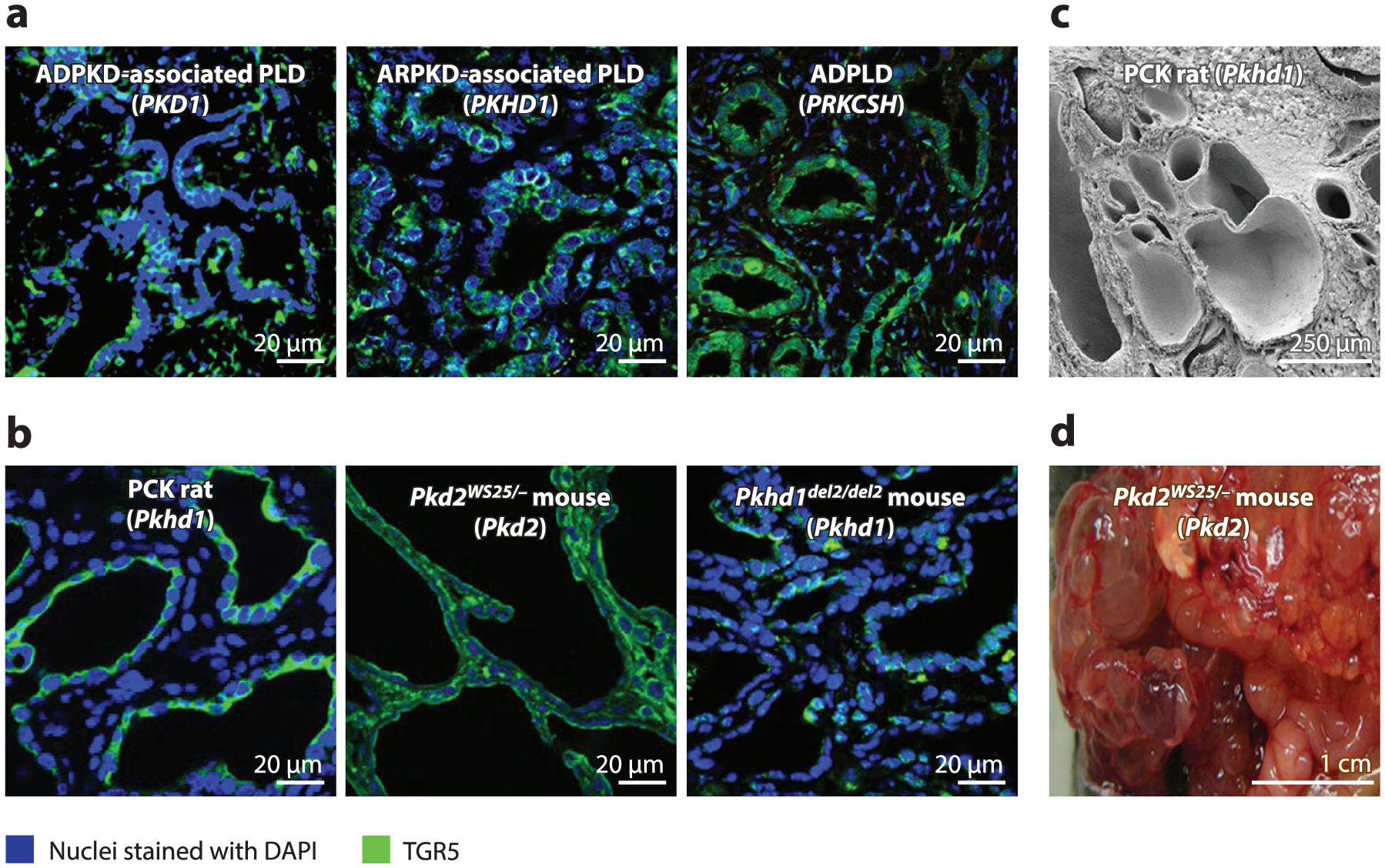
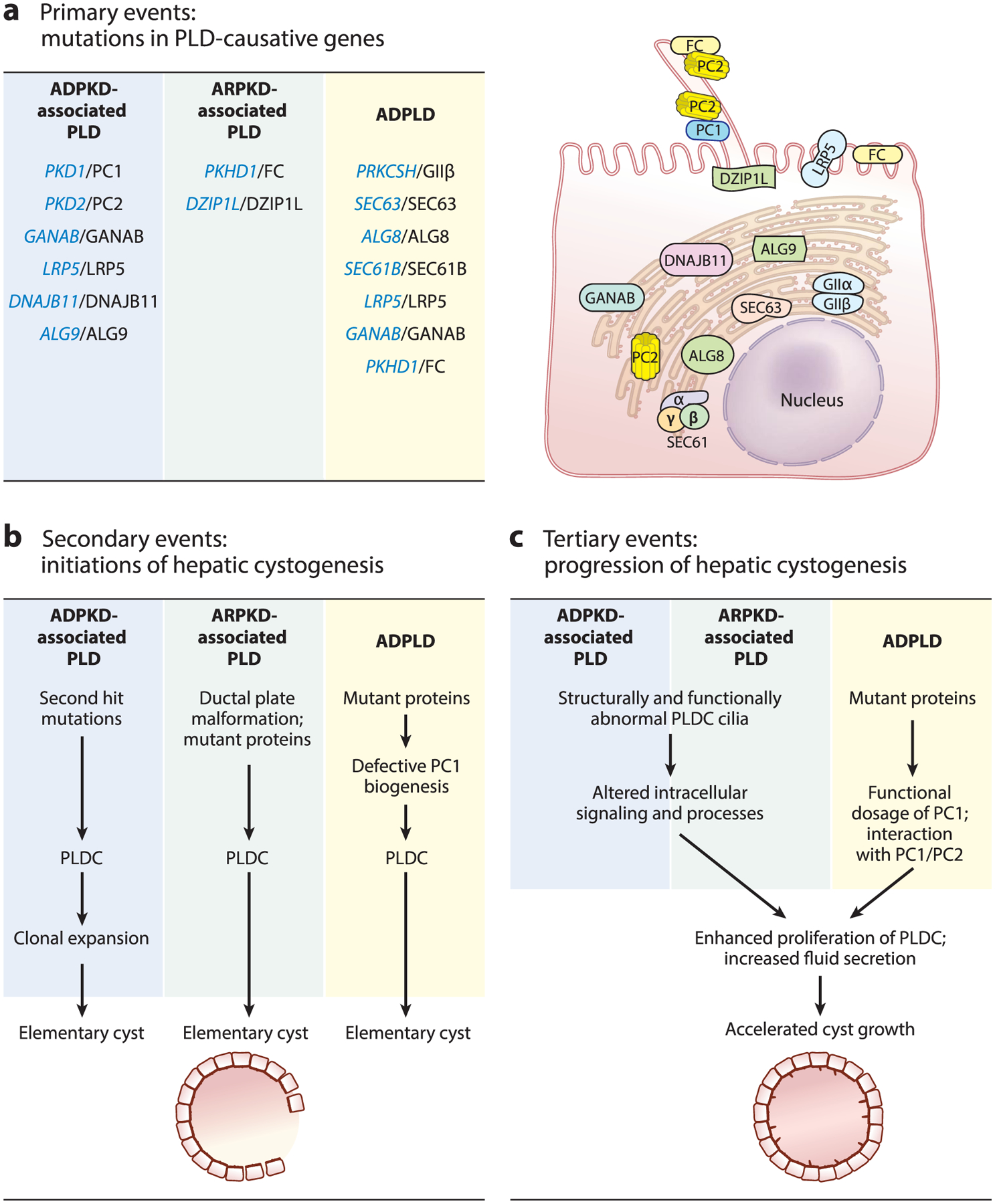
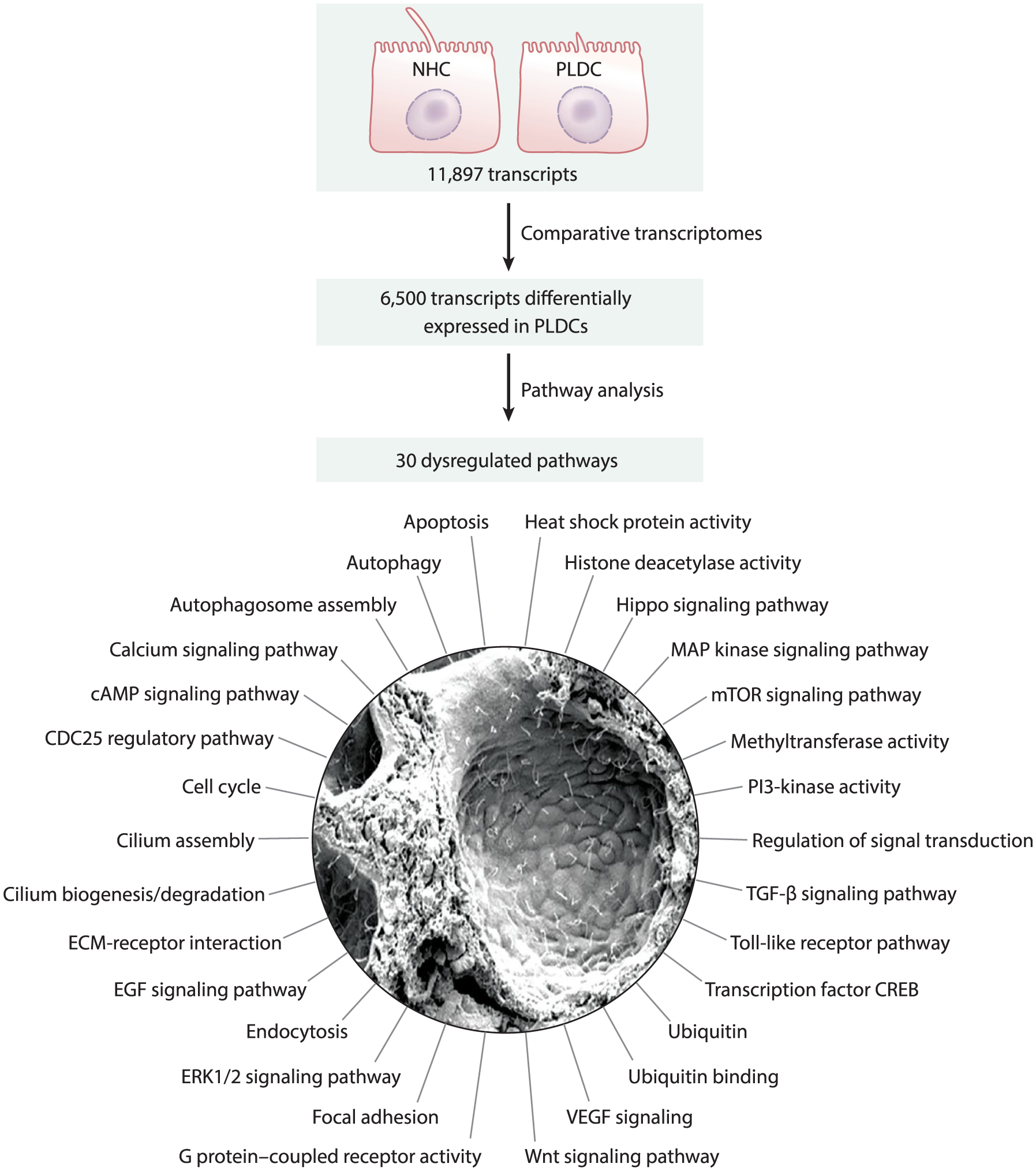
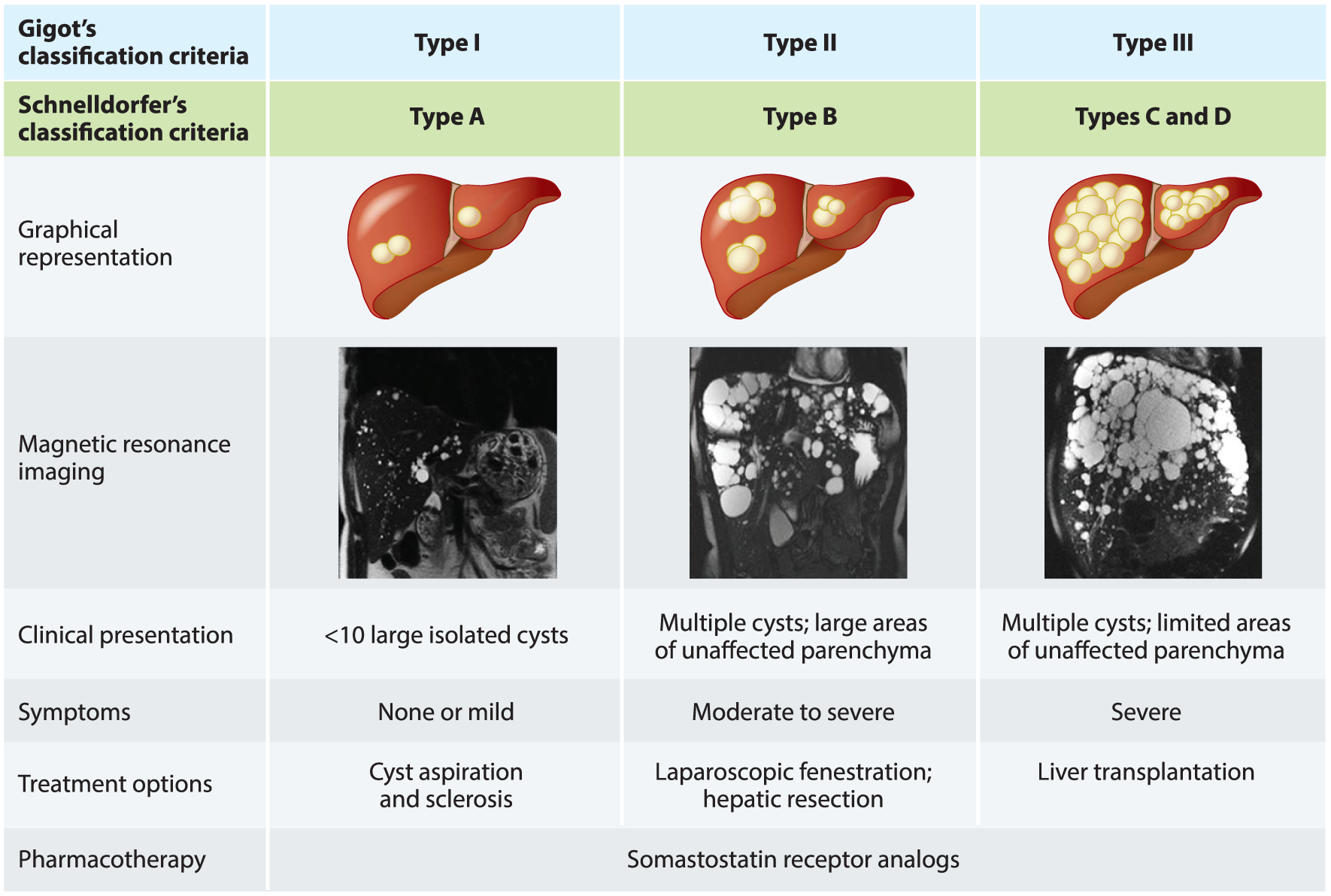
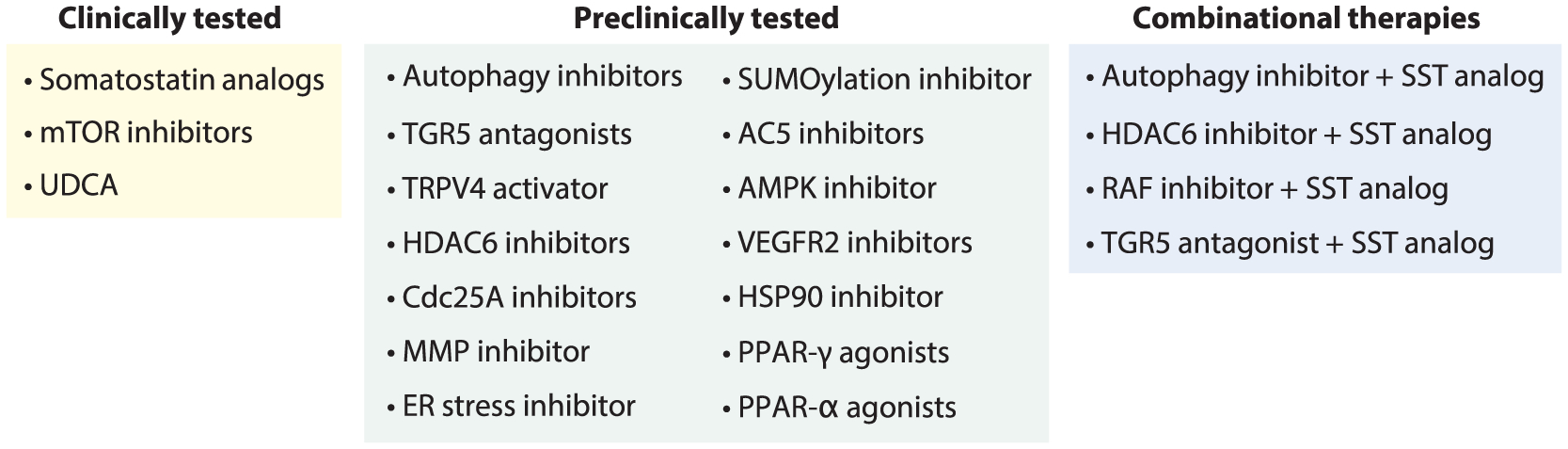
Polycystic liver disease (PLD) is a group of genetic disorders characterized by progressive development of cholangiocyte-derived fluid-filled hepatic cysts. PLD is the most common manifestation of autosomal dominant and autosomal recessive polycystic kidney diseases and rarely occurs as autosomal dominant PLD. The mechanisms of PLD are a sequence of the primary (mutations in PLD-causative genes), secondary (initiation of cyst formation), and tertiary (progression of hepatic cystogenesis) interconnected molecular and cellular events in cholangiocytes. Nonsurgical, surgical, and limited pharmacological treatment options are currently available for clinical management of PLD. Substantial evidence suggests that pharmacological targeting of the signaling pathways and intracellular processes involved in the progression of hepatic cystogenesis is beneficial for PLD. Many of these targets have been evaluated in preclinical and clinical trials. In this review, we discuss the genetic, molecular, and cellular mechanisms of PLD and clinical and preclinical treatment strategies.
Keywords: cholangiocytes; cystogenesis; genetics; mechanisms; polycystic liver disease; therapy.
Figures
References
-
- Norio R 1983. Polycystic disease of liver: an entity of its own or not? Clin. Genet 23:78–79 - PubMed
-
- Barten TRM, Bernts LHP, Drenth JPH, Gevers TJG. 2020. New insights into targeting hepatic cystogenesis in autosomal dominant polycystic liver and kidney disease. Expert Opin. Ther. Targets 24:589–99 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
