

Neuroenhancement of surgeons during robotic suturing
- PMID: 34724587
- PMCID: PMC9160107
- DOI: 10.1007/s00464-021-08823-1
Neuroenhancement of surgeons during robotic suturing
Abstract
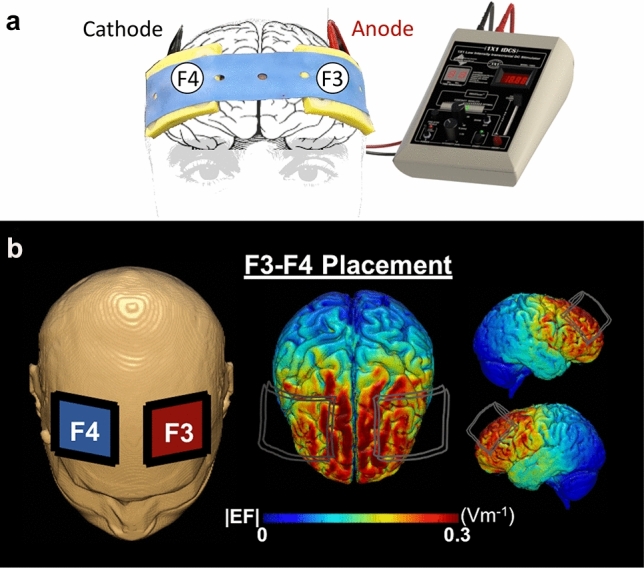
Background: The initial phases of robotic surgical skills acquisition are associated with poor technical performance, such as low knot-tensile strength (KTS). Transcranial direct-current stimulation (tDCS) can improve force and accuracy in motor tasks but research in surgery is limited to open and laparoscopic tasks in students. More recently, robotic surgery has gained traction and is now the most common approach for certain procedures (e.g. prostatectomy). Early-phase robotic suturing performance is dependent on prefrontal cortex (PFC) activation, and this study aimed to determine whether performance can be improved with prefrontal tDCS.
Methods: Fifteen surgical residents were randomized to either active then sham tDCS or sham then active tDCS, in two counterbalanced sessions in a double-blind crossover study. Within each session, participants performed a robotic suturing task repeated in three blocks: pre-, intra- and post-tDCS. During the intra-tDCS block, participants were randomized to either active tDCS (2 mA for 15 min) to the PFC or sham tDCS. Primary outcome measures of technical quality included KTS and error scores.
Results: Significantly faster completion times were observed longitudinally, regardless of active (p < 0.001) or sham stimulation (p < 0.001). KTS was greater following active compared to sham stimulation (median: active = 44.35 N vs. sham = 27.12 N, p < 0.001). A significant reduction in error scores from "pre-" to "post-" (p = 0.029) were only observed in the active group.
Conclusion: tDCS could reduce error and enhance KTS during robotic suturing and warrants further exploration as an adjunct to robotic surgical training.
Keywords: Motor skills; Robotic surgery; Surgical training; Transcranial direct-current stimulation.
© 2021. The Author(s).
Conflict of interest statement
Drs. Ronak Patel, Yusuke Suwa, James Kinross, Alexander von Roon, Adam J Woods, Ara Darzi, Harsimrat Singh and Daniel R Leff have no conflict of interest or financial ties to disclose.
Figures


References
-
- van der Schatte Olivier RH, Van’t Hullenaar CDP, Ruurda JP, Broeders IAMJ (2009) Ergonomics, user comfort, and performance in standard and robot-assisted laparoscopic surgery. Surg Endosc 23(6):1365–1371. http://www.ncbi.nlm.nih.gov/pubmed/18855053. Accessed 2 Jul 2019 - PMC - PubMed
-
- Pernar LIM, Robertson FC, Tavakkoli A, Sheu EG, Brooks DC, Smink DS (2017) An appraisal of the learning curve in robotic general surgery. Surg Endosc 31(31):4583–96. https://link-springer-com.iclibezp1.cc.ic.ac.uk/content/pdf/10.1007%2Fs0.... Accessed 29 May 2019 - PubMed
-
- Herrell SD, Smith JA (2005) Robotic-assisted laparoscopic prostatectomy: what is the learning curve? Urology 66(5):105–107. https://www.sciencedirect.com/science/article/pii/S0090429505009386?via%.... Accessed 2 Jul 2019 - PubMed
-
- Muffly T, McCormick TC, Dean J, Bonham A, Hill RFC (2009) An evaluation of knot integrity when tied robotically and conventionally. Am J Obstet Gynecol 200(5):e18–20. https://linkinghub.elsevier.com/retrieve/pii/S0002937808010272. Accessed 29 May 2019 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
