

Practice patterns and real-life outcomes for patients with acute promyelocytic leukemia in the United States
- PMID: 34724703
- PMCID: PMC8791583
- DOI: 10.1182/bloodadvances.2021005642
Practice patterns and real-life outcomes for patients with acute promyelocytic leukemia in the United States
Abstract
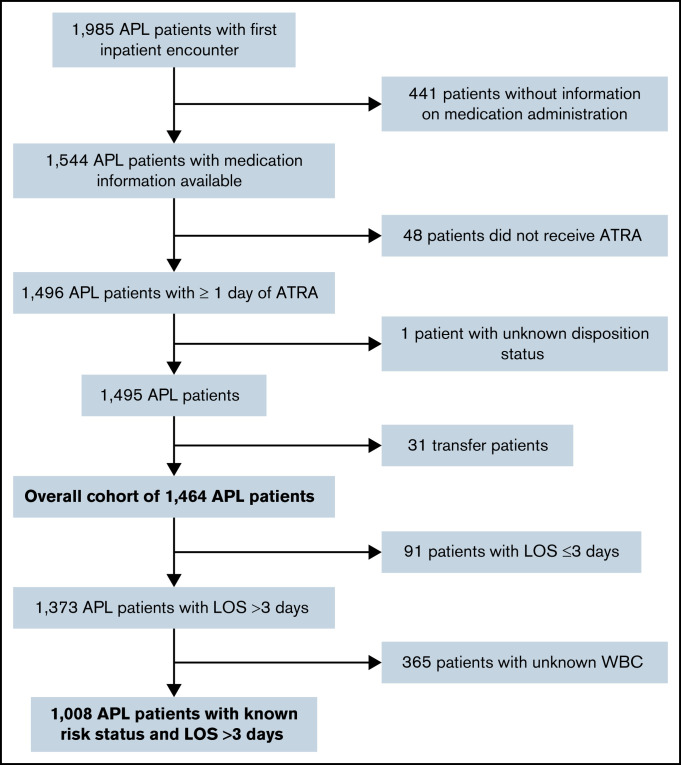
Acute promyelocytic leukemia (APL) is associated with a favorable long-term prognosis if appropriate treatment is initiated promptly. Outcomes in clinical trials and population-based registries vary; potential explanations include a delay in treatment and lower adherence to guideline-recommended therapy in real-world practice. We used the Vizient Clinical Data Base to describe demographic characteristics, baseline clinical characteristics, and treatment patterns in patients newly diagnosed with APL during the study period of April 2017 to March 2020. Baseline white blood cell count was used to assign risk status and assess treatment concordance with National Comprehensive Cancer Network guidelines. Logistic regression models examined adjusted associations between patient, hospital, disease characteristics, and adverse outcomes (in-hospital death or discharge to hospice). Among 1464 patients with APL, 205 (14.0%) experienced an adverse outcome. A substantial subset (20.6%) of patients did not receive guideline-concordant regimens. Odds of adverse outcomes increased with failure to receive guideline-concordant treatment (odds ratio [OR], 2.31; 95% confidence interval [CI], 1.43-3.75; P = .001), high-risk disease (OR, 2.48; 95% CI, 1.53-4.00; P < .001), and increasing age (≥60 years: OR, 11.13; 95% CI, 4.55-27.22; P < .001). Higher hospital acute myeloid leukemia (AML) patient volume was associated with lower odds of adverse outcome (OR, 0.44; 95% CI, 0.20-0.99 [for ≤50 vs >200 AML patients per year]; P = .046). In conclusion, in this large database analysis, 14.0% of patients newly diagnosed with APL died or were discharged to hospice. A substantial proportion of patients did not receive guideline-concordant therapy, potentially contributing to adverse outcomes.
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures


References
-
- Sanz MA, Grimwade D, Tallman MS, et al. Management of acute promyelocytic leukemia: recommendations from an expert panel on behalf of the European LeukemiaNet. Blood. 2009;113(9):1875-1891. - PubMed
-
- Adès L, Guerci A, Raffoux E, et al. ; European APL Group . Very long-term outcome of acute promyelocytic leukemia after treatment with all-trans retinoic acid and chemotherapy: the European APL Group experience. Blood. 2010;115(9):1690-1696. - PubMed
-
- Lo-Coco F, Avvisati G, Vignetti M, et al. ; Study Alliance Leukemia . Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013;369(2):111-121. - PubMed
-
- Zhu HH, Wu DP, Du X, et al. Oral arsenic plus retinoic acid versus intravenous arsenic plus retinoic acid for non-high-risk acute promyelocytic leukaemia: a non-inferiority, randomised phase 3 trial. Lancet Oncol. 2018;19(7):871-879. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
