

Association of clinical competence, specialty and physician country of origin with opioid prescribing for chronic pain: a cohort study
- PMID: 34725228
- PMCID: PMC9046738
- DOI: 10.1136/bmjqs-2021-013503
Association of clinical competence, specialty and physician country of origin with opioid prescribing for chronic pain: a cohort study
Abstract
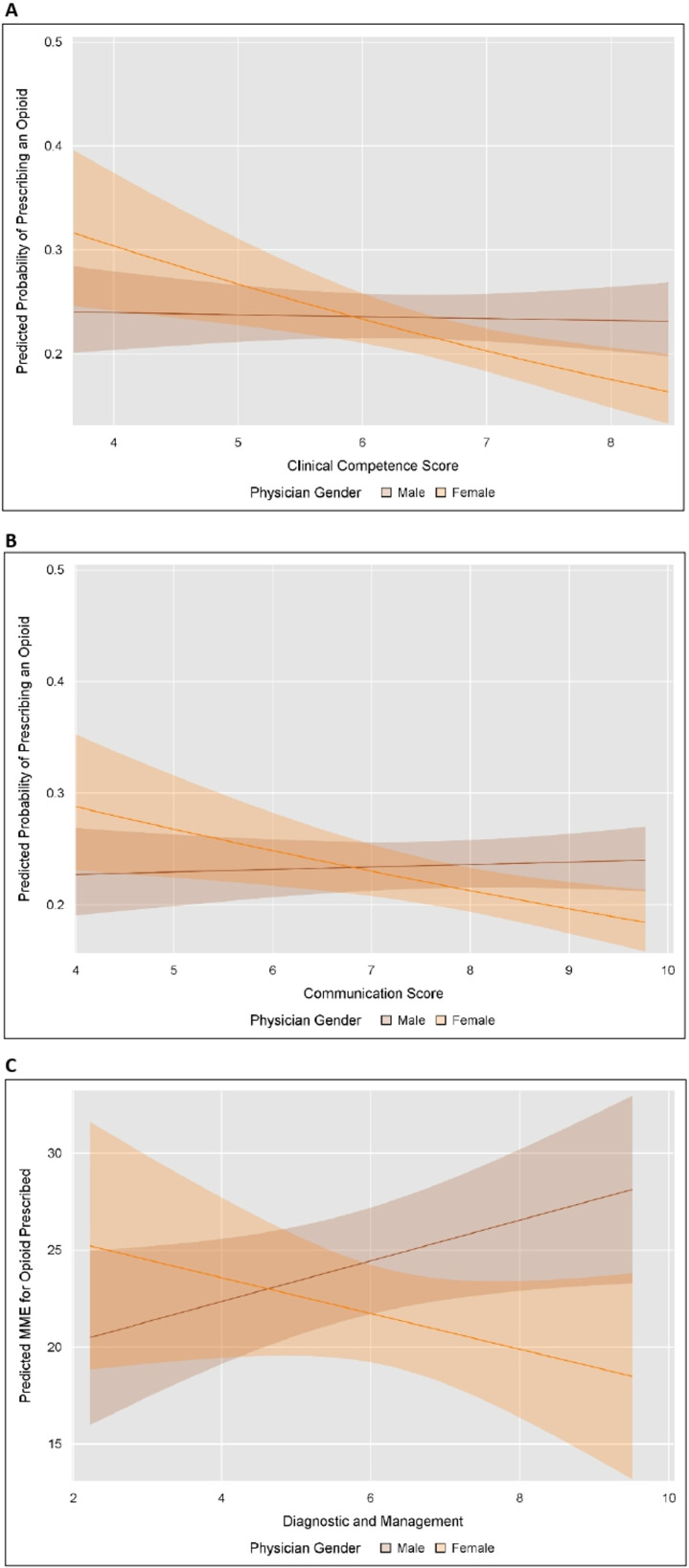
Background: Although little is known about why opioid prescribing practices differ between physicians, clinical competence, specialty training and country of origin may play a role. We hypothesised that physicians with stronger clinical competence and communication skills are less likely to prescribe opioids and prescribe lower doses, as do medical specialists and physicians from Asia.
Methods: Opioid prescribing practices were examined among international medical graduates (IMGs) licensed to practise in the USA who evaluated Medicare patients for chronic pain problems in 2014-2015. Clinical competence was assessed by the Educational Commission for Foreign Medical Graduates (ECFMG) Clinical Skills Assessment. Physicians in the ECFMG database were linked to the American Medical Association Masterfile. Patients evaluated for chronic pain were obtained by linkage to Medicare outpatient and prescription files. Opioid prescribing was measured within 90 days of evaluation visits. Prescribed dose was measured using morphine milligram equivalents (MMEs). Generalised estimating equation logistic and linear regression estimated the association of clinical competence, specialty, and country of origin with opioid prescribing and dose.
Results: 7373 IMGs evaluated 65 012 patients for chronic pain; 15.2% received an opioid prescription. Increased clinical competence was associated with reduced opioid prescribing, but only among female physicians. For every 10% increase in the clinical competence score, the odds of prescribing an opioid decreased by 16% for female physicians (OR 0.84, 95% CI 0.75 to 0.94) but not male physicians (OR 0.99, 95% CI 0.92 to 1.07). Country of origin was associated with prescribed opioid dose; US and Canadian citizens prescribed higher doses (adjusted MME difference +3.56). Primary care physicians were more likely to prescribe opioids, but surgical and hospital-based specialists prescribed higher doses.
Conclusions: Clinical competence at entry into US graduate training, physician gender, specialty and country of origin play a role in opioid prescribing practices.
Keywords: medical education; pain; pharmacoepidemiology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Clinical Knowledge and Trends in Physicians' Prescribing of Opioids for New Onset Back Pain, 2009-2017.JAMA Netw Open. 2021 Jul 1;4(7):e2115328. doi: 10.1001/jamanetworkopen.2021.15328. JAMA Netw Open. 2021. PMID: 34196714 Free PMC article.
-
Changes in Initial Opioid Prescribing Practices After the 2016 Release of the CDC Guideline for Prescribing Opioids for Chronic Pain.JAMA Netw Open. 2021 Jul 1;4(7):e2116860. doi: 10.1001/jamanetworkopen.2021.16860. JAMA Netw Open. 2021. PMID: 34255047 Free PMC article.
-
Differential prescribing of opioid analgesics according to physician specialty for Medicaid patients with chronic noncancer pain diagnoses.Pain Res Manag. 2014 Jul-Aug;19(4):179-85. doi: 10.1155/2014/857952. Epub 2014 May 7. Pain Res Manag. 2014. PMID: 24809067 Free PMC article.
-
Clinical Decision Support Systems for Opioid Prescribing for Chronic Non-Cancer Pain in Primary Care: A Scoping Review.J Am Board Fam Med. 2020 Jul-Aug;33(4):529-540. doi: 10.3122/jabfm.2020.04.190199. J Am Board Fam Med. 2020. PMID: 32675264
-
Competence and confidence with prescribing in pharmacy and medicine: a scoping review.Int J Pharm Pract. 2020 Aug;28(4):312-325. doi: 10.1111/ijpp.12595. Epub 2019 Dec 25. Int J Pharm Pract. 2020. PMID: 31876027
Cited by
-
Clinical competence, communication ability and adherence to choosing wisely recommendations for lipid reducing drug use in older adults.BMC Geriatr. 2023 Nov 20;23(1):761. doi: 10.1186/s12877-023-04429-5. BMC Geriatr. 2023. PMID: 37986045 Free PMC article.
-
Understanding general practitioners' prescribing choices to patients with chronic low back pain: a discrete choice experiment.Int J Clin Pharm. 2024 Feb;46(1):111-121. doi: 10.1007/s11096-023-01649-y. Epub 2023 Oct 26. Int J Clin Pharm. 2024. PMID: 37882955 Free PMC article.
-
Does Physicians' Clinical Competence, Communication Ability, or Cultural Background Influence Potentially Inappropriate Prescribing of Benzodiazepines and Z-Drugs Among Older Adults With Insomnia?Pharmacoepidemiol Drug Saf. 2024 Dec;33(12):e70068. doi: 10.1002/pds.70068. Pharmacoepidemiol Drug Saf. 2024. PMID: 39628100 Free PMC article.
-
Exploring Factors Associated with Prescribers' Comfort Levels in Analgesic Prescribing in Quebec.J Pain Res. 2024 Aug 16;17:2667-2677. doi: 10.2147/JPR.S469052. eCollection 2024. J Pain Res. 2024. PMID: 39165720 Free PMC article.
-
Opioid use in postoperative pain management of pediatric appendectomy patients in Japan.J Anesth. 2025 Jun 14. doi: 10.1007/s00540-025-03525-7. Online ahead of print. J Anesth. 2025. PMID: 40515766
References
-
- CDC . Drug overdose deaths: centers for disease control and prevention (CDC), 2020. Available: https://www.cdc.gov/drugoverdose/data/statedeaths.html [Accessed 22 Oct 2020].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous