

Assessing cost-effectiveness of hepatitis C testing pathways in Georgia using the Hep C Testing Calculator
- PMID: 34725356
- PMCID: PMC8560949
- DOI: 10.1038/s41598-021-00362-y
Assessing cost-effectiveness of hepatitis C testing pathways in Georgia using the Hep C Testing Calculator
Erratum in
-
Author Correction: Assessing cost-effectiveness of hepatitis C testing pathways in Georgia using the Hep C Testing Calculator.Sci Rep. 2022 Feb 17;12(1):3101. doi: 10.1038/s41598-022-07001-0. Sci Rep. 2022. PMID: 35177757 Free PMC article. No abstract available.
Abstract
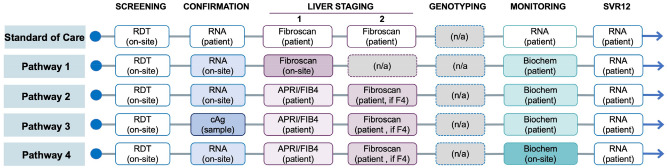
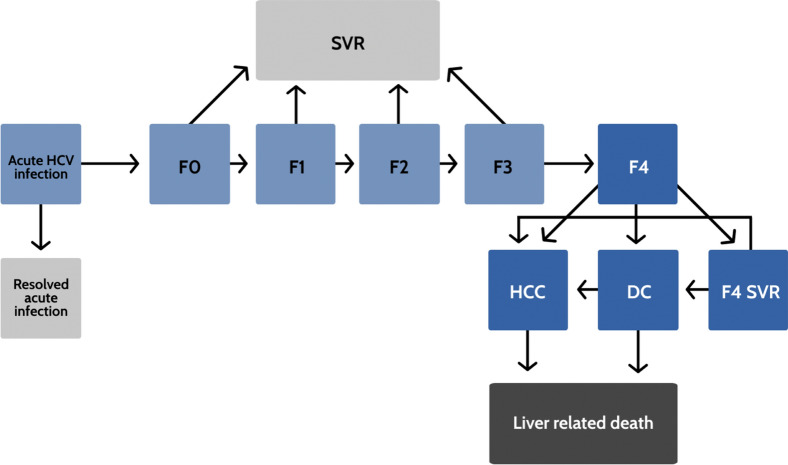
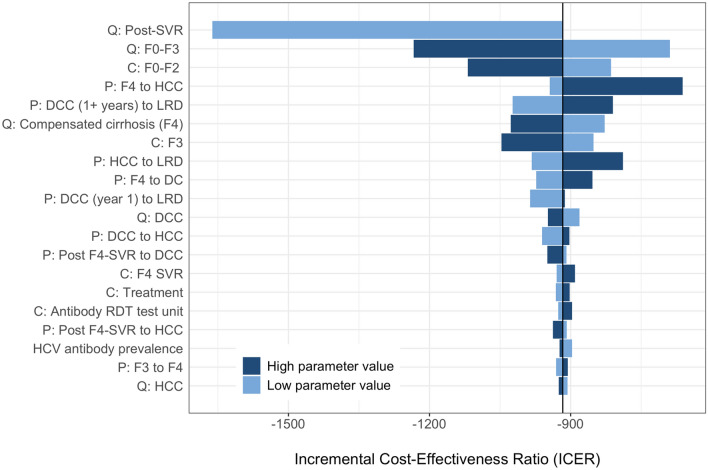
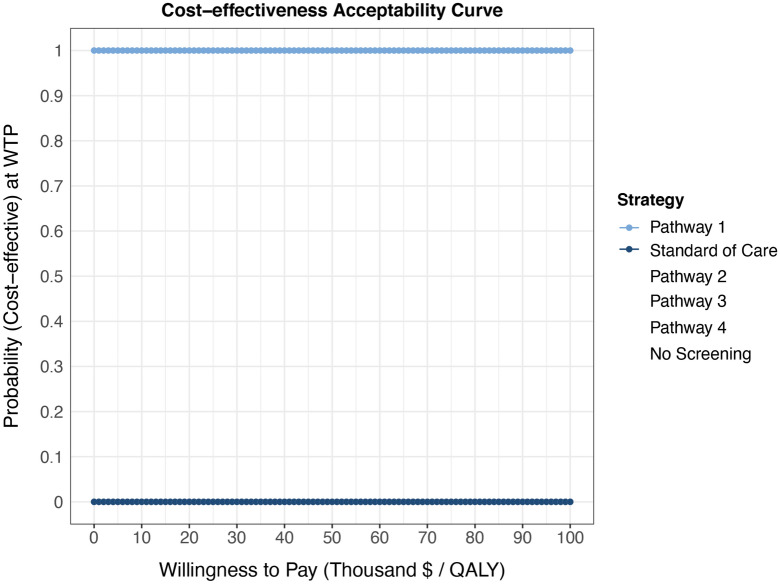
The cost of testing can be a substantial contributor to hepatitis C virus (HCV) elimination program costs in many low- and middle-income countries such as Georgia, resulting in the need for innovative and cost-effective strategies for testing. Our objective was to investigate the most cost-effective testing pathways for scaling-up HCV testing in Georgia. We developed a Markov-based model with a lifetime horizon that simulates the natural history of HCV, and the cost of detection and treatment of HCV. We then created an interactive online tool that uses results from the Markov-based model to evaluate the cost-effectiveness of different HCV testing pathways. We compared the current standard-of-care (SoC) testing pathway and four innovative testing pathways for Georgia. The SoC testing was cost-saving compared to no testing, but all four new HCV testing pathways further increased QALYs and decreased costs. The pathway with the highest patient follow-up, due to on-site testing, resulted in the highest discounted QALYs (123 QALY more than the SoC) and lowest costs ($127,052 less than the SoC) per 10,000 persons screened. The current testing algorithm in Georgia can be replaced with a new pathway that is more effective while being cost-saving.
© 2021. The Author(s).
Conflict of interest statement
S. Shilton is an employee of The Foundation for Innovative New Diagnostics. Dr. Chhatwal reported receiving grants from the National Science Foundation and Unitaid during the conduct of the study, grants and personal fees from Gilead and Merck & Co outside the submitted work, and served as a partner with Value Analytics Labs outside the submitted work. All other authors have no competing/conflict of interest.
Figures
References
-
- World Health Organization. Global Hepatitis Report (2017).
-
- World Health Organization. Combating hepatitis B and C to reach elimination by 2030 (2016).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
