

Cardiovascular morbidities in postoperative colorectal cancer patients
- PMID: 34725390
- PMCID: PMC8560922
- DOI: 10.1038/s41598-021-00735-3
Cardiovascular morbidities in postoperative colorectal cancer patients
Abstract
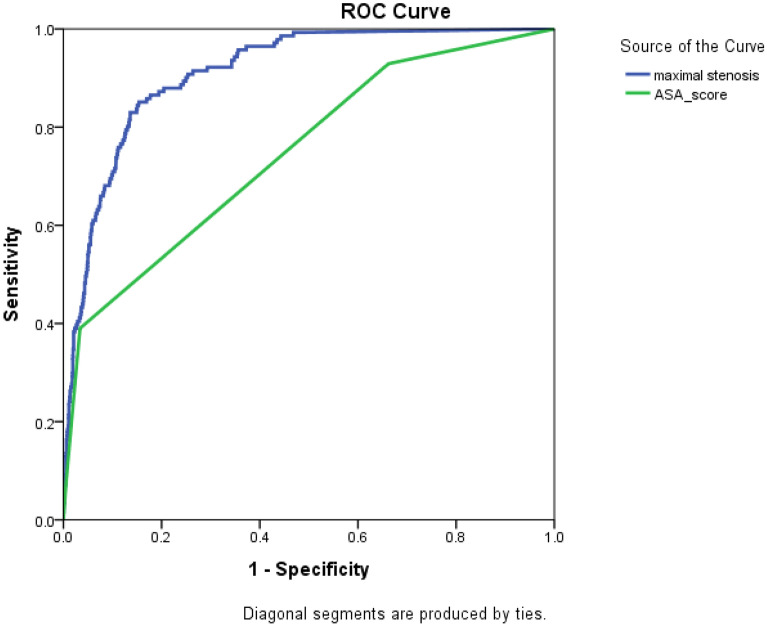
This retrospective observational study investigated the long-term prevalence of new-onset cardiovascular disease (CVD) and the predictive role of atherosclerotic plaque in the aorta and iliac arteries for CVD in postoperative colorectal cancer (CRC) patients who received surgical treatment between 2014 and 2015. CVD included coronary or cerebrovascular diseases which required treatment and new-onset CVD included peri-and postoperatively diagnosed CVDs or aggravated CVDs that required additional treatment during follow-up. Of the 2,875 patients included in this study, the prevalence of CVD was 8.9% (255/2875) and 141 (4.9%) developed new-onset CVD. Maximum arterial stenosis in the aorta or iliac arteries occurred in 40.8 ± 18.6% of patients with new-onset CVD and 11.6 ± 13.8% of patients without new-onset CVD (p < 0.001). The mean new-onset CVD-free survival time in patients with > 30% and < 30% stenoses were 52.5 [95% confidence intervals (CIs) 50.0-54.9] and 66.5 (95% CIs 66.2-66.8) months, respectively (p < 0.001). The area under the receiver operating characteristic curve of the maximal arterial stenosis for new-onset CVD was 0.911. These results suggest that CRC patients are at risk for developing new-onset CVD, which is associated with reduced survival. Atherosclerotic burden in the aorta or both iliac arteries may help predict future CVD events.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Wang H, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1459–1544. doi: 10.1016/S0140-6736(16)31012-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
