

Improved prediction of immune checkpoint blockade efficacy across multiple cancer types
- PMID: 34725502
- PMCID: PMC9363980
- DOI: 10.1038/s41587-021-01070-8
Improved prediction of immune checkpoint blockade efficacy across multiple cancer types
Abstract
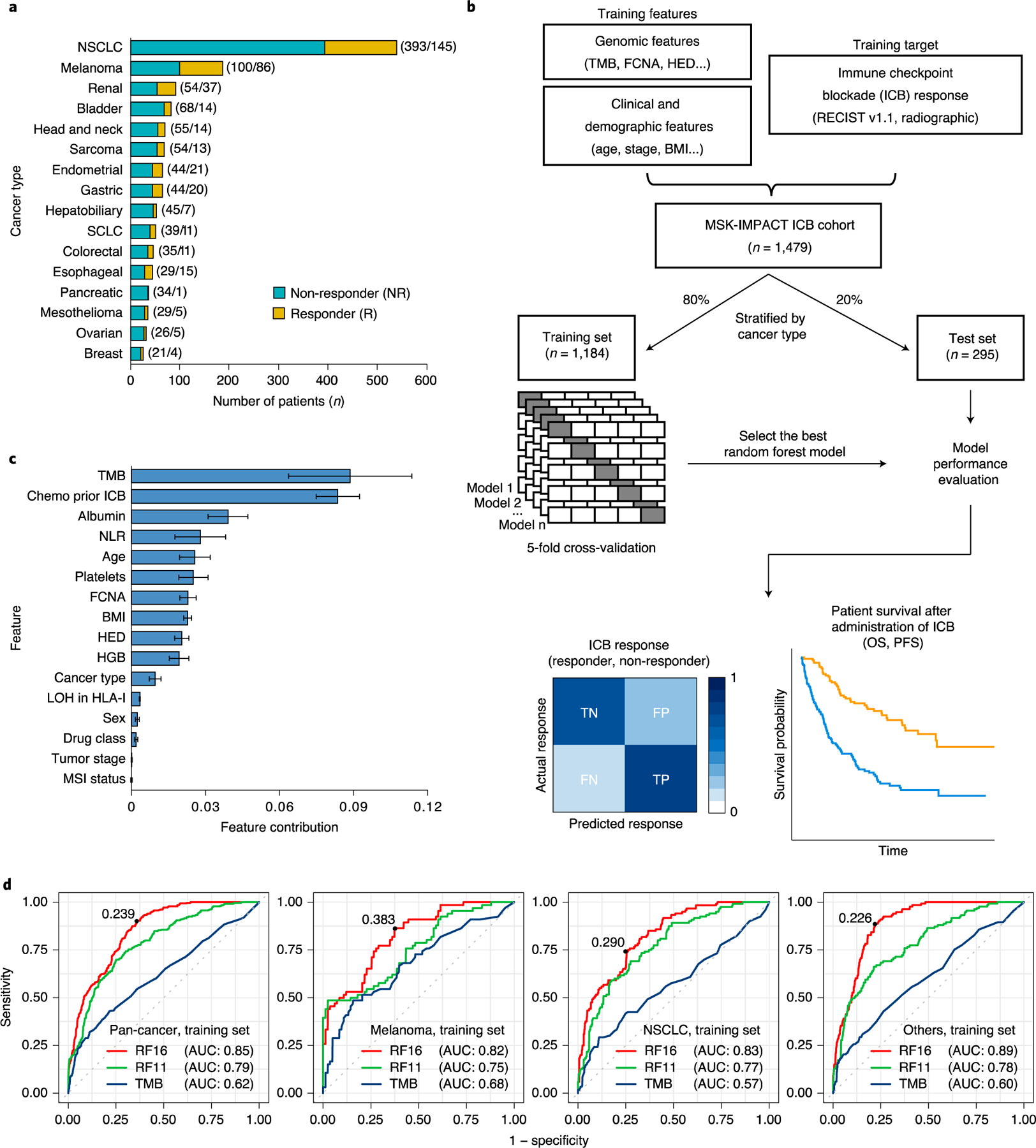
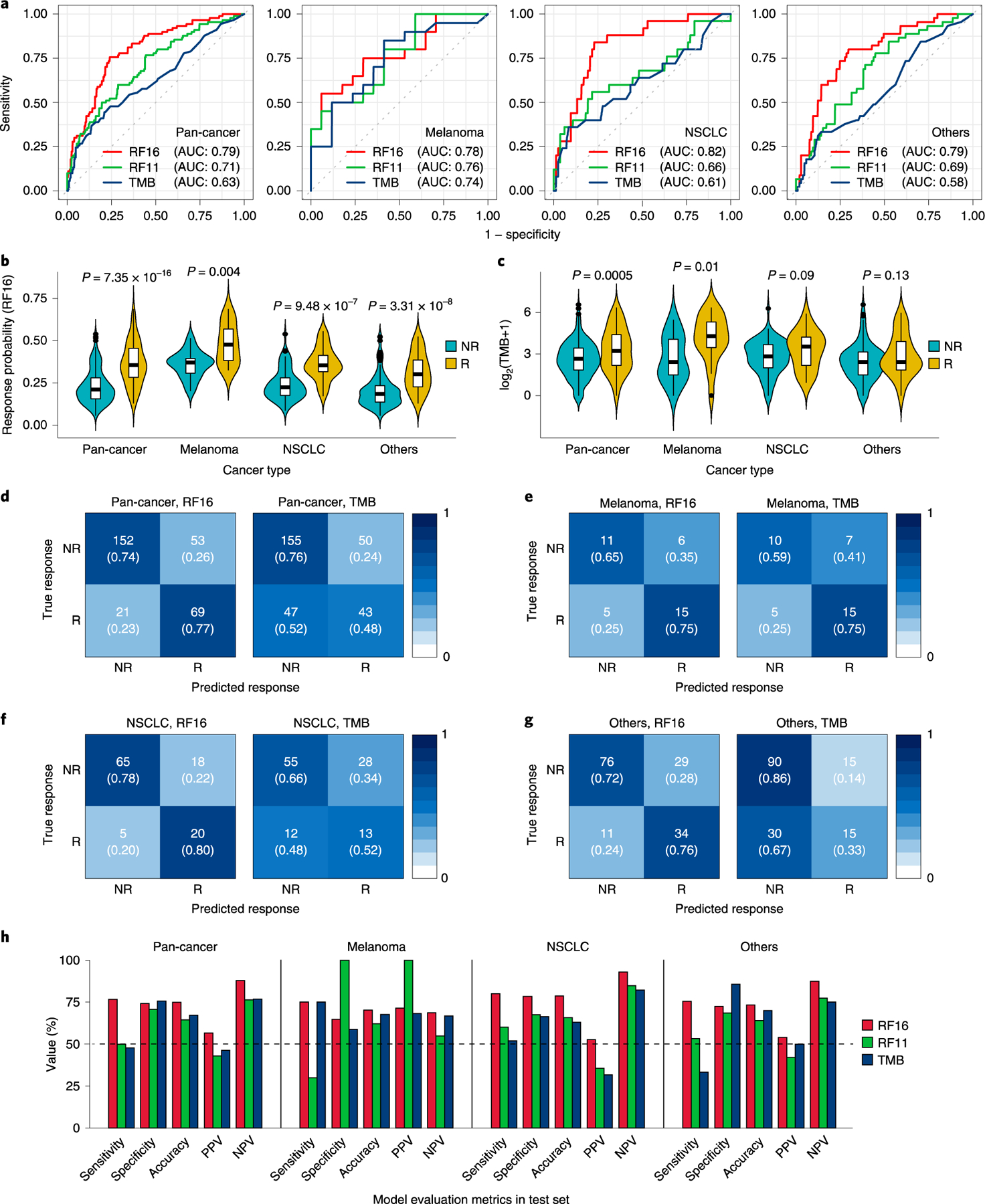
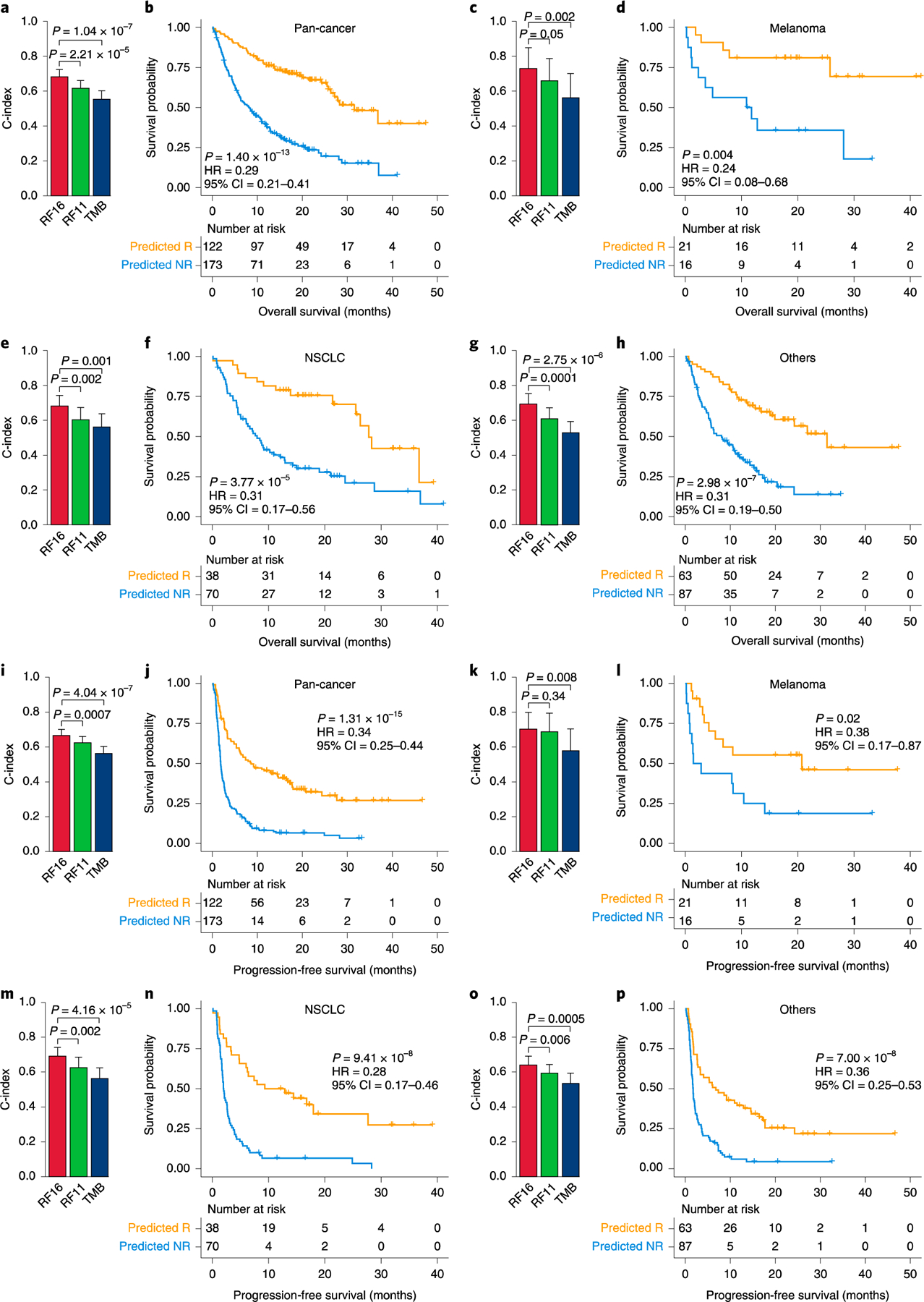
Only a fraction of patients with cancer respond to immune checkpoint blockade (ICB) treatment, but current decision-making procedures have limited accuracy. In this study, we developed a machine learning model to predict ICB response by integrating genomic, molecular, demographic and clinical data from a comprehensively curated cohort (MSK-IMPACT) with 1,479 patients treated with ICB across 16 different cancer types. In a retrospective analysis, the model achieved high sensitivity and specificity in predicting clinical response to immunotherapy and predicted both overall survival and progression-free survival in the test data across different cancer types. Our model significantly outperformed predictions based on tumor mutational burden, which was recently approved by the U.S. Food and Drug Administration for this purpose1. Additionally, the model provides quantitative assessments of the model features that are most salient for the predictions. We anticipate that this approach will substantially improve clinical decision-making in immunotherapy and inform future interventions.
© 2021. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests
T.A.C. is a co-founder of Gritstone Oncology and holds equity. T.A.C. holds equity in An2H. T.A.C. acknowledges grant funding from Bristol Myers Squibb, AstraZeneca, Illumina, Pfizer, An2H and Eisai. T.A.C. has served as an advisor for Bristol Myers, Medlmmune, Squibb, Illumina, Eisai, AstraZeneca and An2H. T.A.C., L.G.T.M. and D.C. hold ownership of intellectual property on using tumor mutational burden to predict immunotherapy response, with a pending patent, which has been licensed to PGDx. M.A.P. reports consulting fees from Bristol Myers Squibb, Merck, Array BioPharma, Novartis, Incyte, NewLink Genetics, Aduro and Eisai; honoraria from Bristol Myers Squibb and Merck; and institutional support from RGenix, Infinity, Bristol Myers Squibb, Merck, Array BioPharma, Novartis and AstraZeneca. M.L. has received advisory board compensation from Merck and Bristol Myers Squibb. The remaining authors declare no competing interests.
Figures
References
-
- Subbiah V, Solit DB, Chan TA & Kurzrock R The FDA approval of pembrolizumab for adult and pediatric patients with tumor mutational burden (TMB) ≥10: a decision centered on empowering patients and their physicians. Ann. Oncol 31, 1115–1118 (2020). - PubMed
-
- Bendell J et al. Efficacy and safety results from IMblaze370, a randomised phase III study comparing atezolizumab plus cobimetinib and atezolizumab monotherapy vs regorafenib in chemotherapy-refractory metastatic colorectal cancer. Ann. Oncol 29, 123–123 (2018).
-
- Cohen EE et al. Pembrolizumab (pembro) vs standard of care (SOC) for recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC): phase 3 KEYNOTE-040 trial. Ann. Oncol 28 https://oncologypro.esmo.org/meeting-resources/esmo-2017-congress/Pembro... (2017).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
