

Exploratory Data Mining Techniques (Decision Tree Models) for Examining the Impact of Internet-Based Cognitive Behavioral Therapy for Tinnitus: Machine Learning Approach
- PMID: 34726612
- PMCID: PMC8596228
- DOI: 10.2196/28999
Exploratory Data Mining Techniques (Decision Tree Models) for Examining the Impact of Internet-Based Cognitive Behavioral Therapy for Tinnitus: Machine Learning Approach
Abstract
Background: There is huge variability in the way that individuals with tinnitus respond to interventions. These experiential variations, together with a range of associated etiologies, contribute to tinnitus being a highly heterogeneous condition. Despite this heterogeneity, a "one size fits all" approach is taken when making management recommendations. Although there are various management approaches, not all are equally effective. Psychological approaches such as cognitive behavioral therapy have the most evidence base. Managing tinnitus is challenging due to the significant variations in tinnitus experiences and treatment successes. Tailored interventions based on individual tinnitus profiles may improve outcomes. Predictive models of treatment success are, however, lacking.
Objective: This study aimed to use exploratory data mining techniques (ie, decision tree models) to identify the variables associated with the treatment success of internet-based cognitive behavioral therapy (ICBT) for tinnitus.
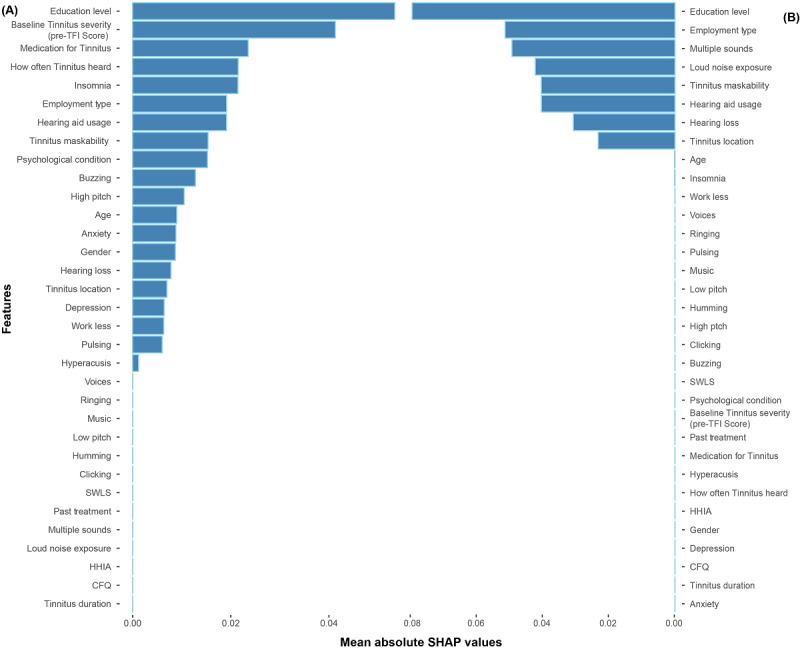
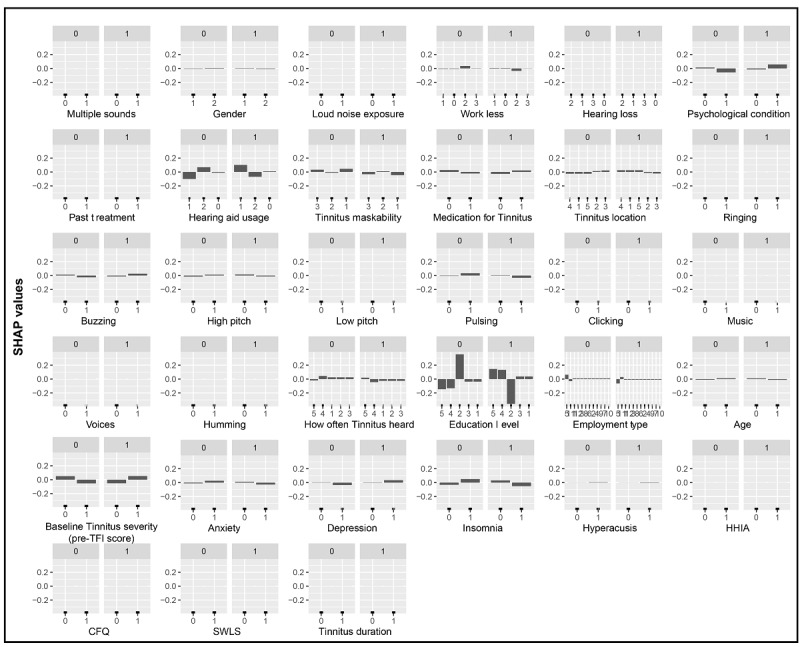
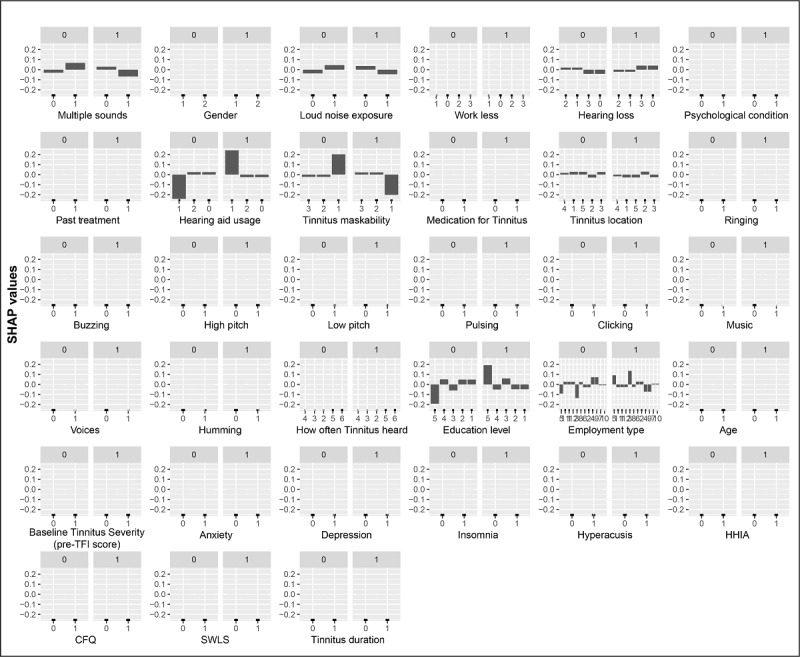
Methods: Individuals (N=228) who underwent ICBT in 3 separate clinical trials were included in this analysis. The primary outcome variable was a reduction of 13 points in tinnitus severity, which was measured by using the Tinnitus Functional Index following the intervention. The predictor variables included demographic characteristics, tinnitus and hearing-related variables, and clinical factors (ie, anxiety, depression, insomnia, hyperacusis, hearing disability, cognitive function, and life satisfaction). Analyses were undertaken by using various exploratory machine learning algorithms to identify the most influencing variables. In total, 6 decision tree models were implemented, namely the classification and regression tree (CART), C5.0, GB, XGBoost, AdaBoost algorithm and random forest models. The Shapley additive explanations framework was applied to the two optimal decision tree models to determine relative predictor importance.
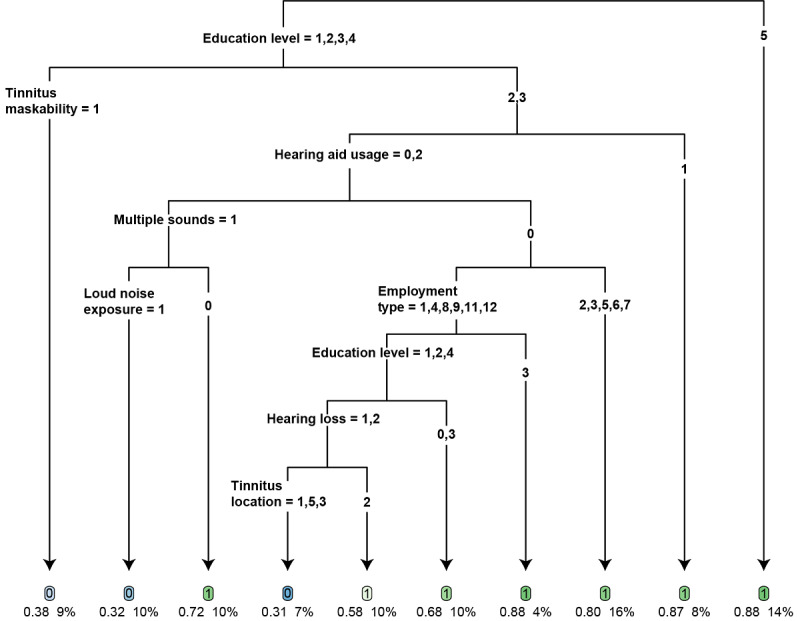
Results: Among the six decision tree models, the CART (accuracy: mean 70.7%, SD 2.4%; sensitivity: mean 74%, SD 5.5%; specificity: mean 64%, SD 3.7%; area under the receiver operating characteristic curve [AUC]: mean 0.69, SD 0.001) and gradient boosting (accuracy: mean 71.8%, SD 1.5%; sensitivity: mean 78.3%, SD 2.8%; specificity: 58.7%, SD 4.2%; AUC: mean 0.68, SD 0.02) models were found to be the best predictive models. Although the other models had acceptable accuracy (range 56.3%-66.7%) and sensitivity (range 68.6%-77.9%), they all had relatively weak specificity (range 31.1%-50%) and AUCs (range 0.52-0.62). A higher education level was the most influencing factor for ICBT outcomes. The CART decision tree model identified 3 participant groups who had at least an 85% success probability following the undertaking of ICBT.
Conclusions: Decision tree models, especially the CART and gradient boosting models, appeared to be promising in predicting ICBT outcomes. Their predictive power may be improved by using larger sample sizes and including a wider range of predictive factors in future studies.
Keywords: artificial intelligence; cognitive behavioral therapy; data mining; decision tree; digital therapeutics; internet interventions; machine learning; random forest; tinnitus.
©Hansapani Rodrigo, Eldré W Beukes, Gerhard Andersson, Vinaya Manchaiah. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 02.11.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Predicting the Outcomes of Internet-Based Cognitive Behavioral Therapy for Tinnitus: Applications of Artificial Neural Network and Support Vector Machine.Am J Audiol. 2022 Dec 5;31(4):1167-1177. doi: 10.1044/2022_AJA-21-00270. Epub 2022 Oct 10. Am J Audiol. 2022. PMID: 36215687 Free PMC article.
-
Dismantling internet-based cognitive behavioral therapy for tinnitus. The contribution of applied relaxation: A randomized controlled trial.Internet Interv. 2021 May 12;25:100402. doi: 10.1016/j.invent.2021.100402. eCollection 2021 Sep. Internet Interv. 2021. PMID: 34040997 Free PMC article.
-
Internet-Based Intervention for Tinnitus: Outcome of a Single-Group Open Trial.J Am Acad Audiol. 2017 Apr;28(4):340-351. doi: 10.3766/jaaa.16055. J Am Acad Audiol. 2017. PMID: 28418328
-
Internet-based cognitive behavioral therapy for patients with chronic somatic conditions: a meta-analytic review.J Med Internet Res. 2014 Mar 27;16(3):e88. doi: 10.2196/jmir.2777. J Med Internet Res. 2014. PMID: 24675372 Free PMC article. Review.
-
Internet-Delivered Psychological Treatments for Tinnitus: A Brief Historical Review.Am J Audiol. 2022 Sep 21;31(3S):1013-1018. doi: 10.1044/2022_AJA-21-00245. Epub 2022 Apr 20. Am J Audiol. 2022. PMID: 35442718 Review.
Cited by
-
Cognitive Behavioural Therapy (CBT) for Managing Tinnitus, Hyperacusis, and Misophonia: The 2025 Tonndorf Lecture.Brain Sci. 2025 May 19;15(5):526. doi: 10.3390/brainsci15050526. Brain Sci. 2025. PMID: 40426697 Free PMC article.
-
Juxtaposing Medical Centers Using Different Questionnaires Through Score Predictors.Front Neurosci. 2022 Mar 23;16:818686. doi: 10.3389/fnins.2022.818686. eCollection 2022. Front Neurosci. 2022. PMID: 35401072 Free PMC article.
-
Machine learning-based gait adaptation dysfunction identification using CMill-based gait data.Front Neurorobot. 2024 Jul 29;18:1421401. doi: 10.3389/fnbot.2024.1421401. eCollection 2024. Front Neurorobot. 2024. PMID: 39136036 Free PMC article.
-
Explainable AI Method for Tinnitus Diagnosis via Neighbor-Augmented Knowledge Graph and Traditional Chinese Medicine: Development and Validation Study.JMIR Med Inform. 2024 Jun 10;12:e57678. doi: 10.2196/57678. JMIR Med Inform. 2024. PMID: 38857077 Free PMC article.
-
Optimizing age-related hearing risk predictions: an advanced machine learning integration with HHIE-S.BioData Min. 2023 Dec 14;16(1):35. doi: 10.1186/s13040-023-00351-z. BioData Min. 2023. PMID: 38098102 Free PMC article.
References
-
- McCormack A, Edmondson-Jones M, Somerset S, Hall D. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. 2016 Jul;337:70–79. doi: 10.1016/j.heares.2016.05.009. https://linkinghub.elsevier.com/retrieve/pii/S0378-5955(16)30027-2 S0378-5955(16)30027-2 - DOI - PubMed
-
- Kim HJ, Lee HJ, An SY, Sim S, Park B, Kim SW, Lee JS, Hong SK, Choi HG. Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS One. 2015 May 28;10(5):e0127578. doi: 10.1371/journal.pone.0127578. https://dx.plos.org/10.1371/journal.pone.0127578 PONE-D-14-41251 - DOI - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
