

Effect of Amoxicillin Dose and Treatment Duration on the Need for Antibiotic Re-treatment in Children With Community-Acquired Pneumonia: The CAP-IT Randomized Clinical Trial
- PMID: 34726708
- PMCID: PMC8564579
- DOI: 10.1001/jama.2021.17843
Effect of Amoxicillin Dose and Treatment Duration on the Need for Antibiotic Re-treatment in Children With Community-Acquired Pneumonia: The CAP-IT Randomized Clinical Trial
Erratum in
-
Misspelled Surname.JAMA. 2021 Dec 7;326(21):2208. doi: 10.1001/jama.2021.20219. JAMA. 2021. PMID: 34874442 Free PMC article. No abstract available.
Abstract
Importance: The optimal dose and duration of oral amoxicillin for children with community-acquired pneumonia (CAP) are unclear.
Objective: To determine whether lower-dose amoxicillin is noninferior to higher dose and whether 3-day treatment is noninferior to 7 days.
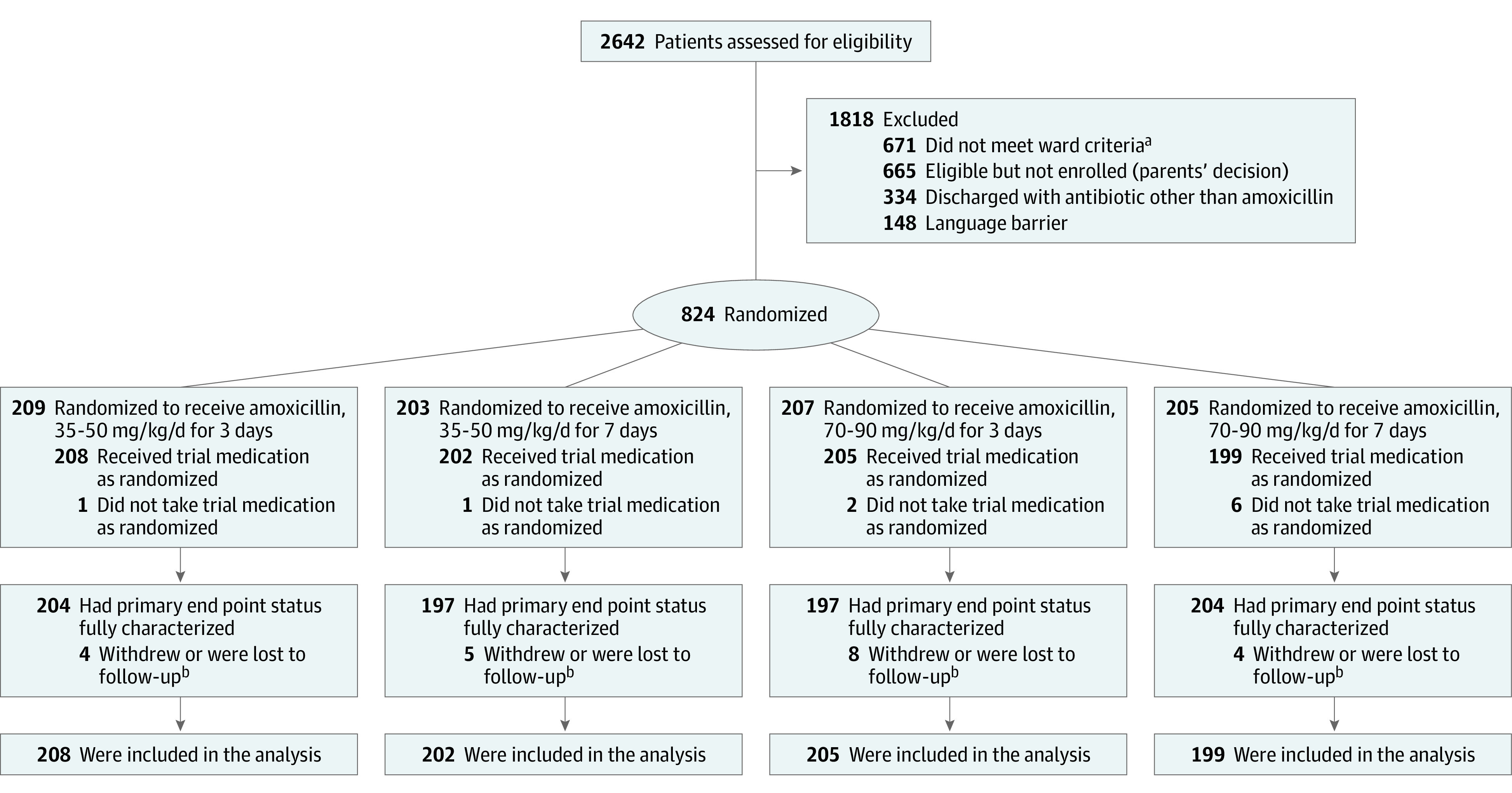
Design, setting, and participants: Multicenter, randomized, 2 × 2 factorial noninferiority trial enrolling 824 children, aged 6 months and older, with clinically diagnosed CAP, treated with amoxicillin on discharge from emergency departments and inpatient wards of 28 hospitals in the UK and 1 in Ireland between February 2017 and April 2019, with last trial visit on May 21, 2019.
Interventions: Children were randomized 1:1 to receive oral amoxicillin at a lower dose (35-50 mg/kg/d; n = 410) or higher dose (70-90 mg/kg/d; n = 404), for a shorter duration (3 days; n = 413) or a longer duration (7 days; n = 401).
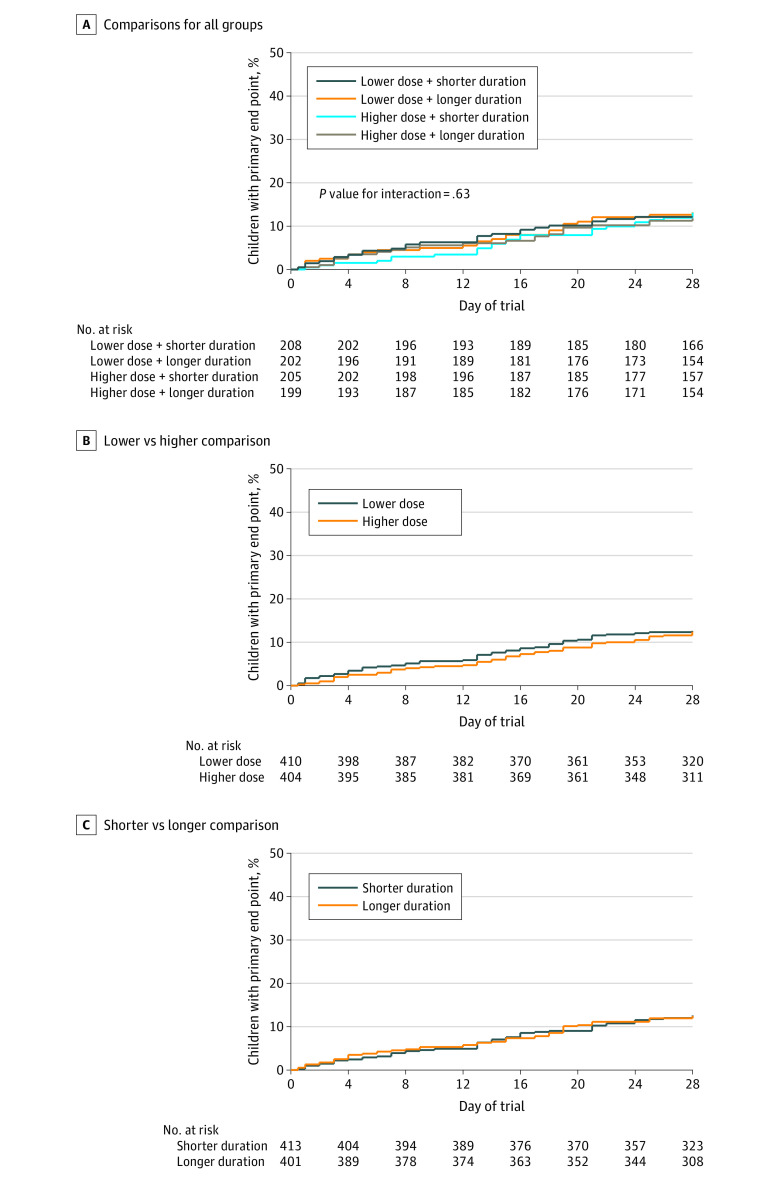
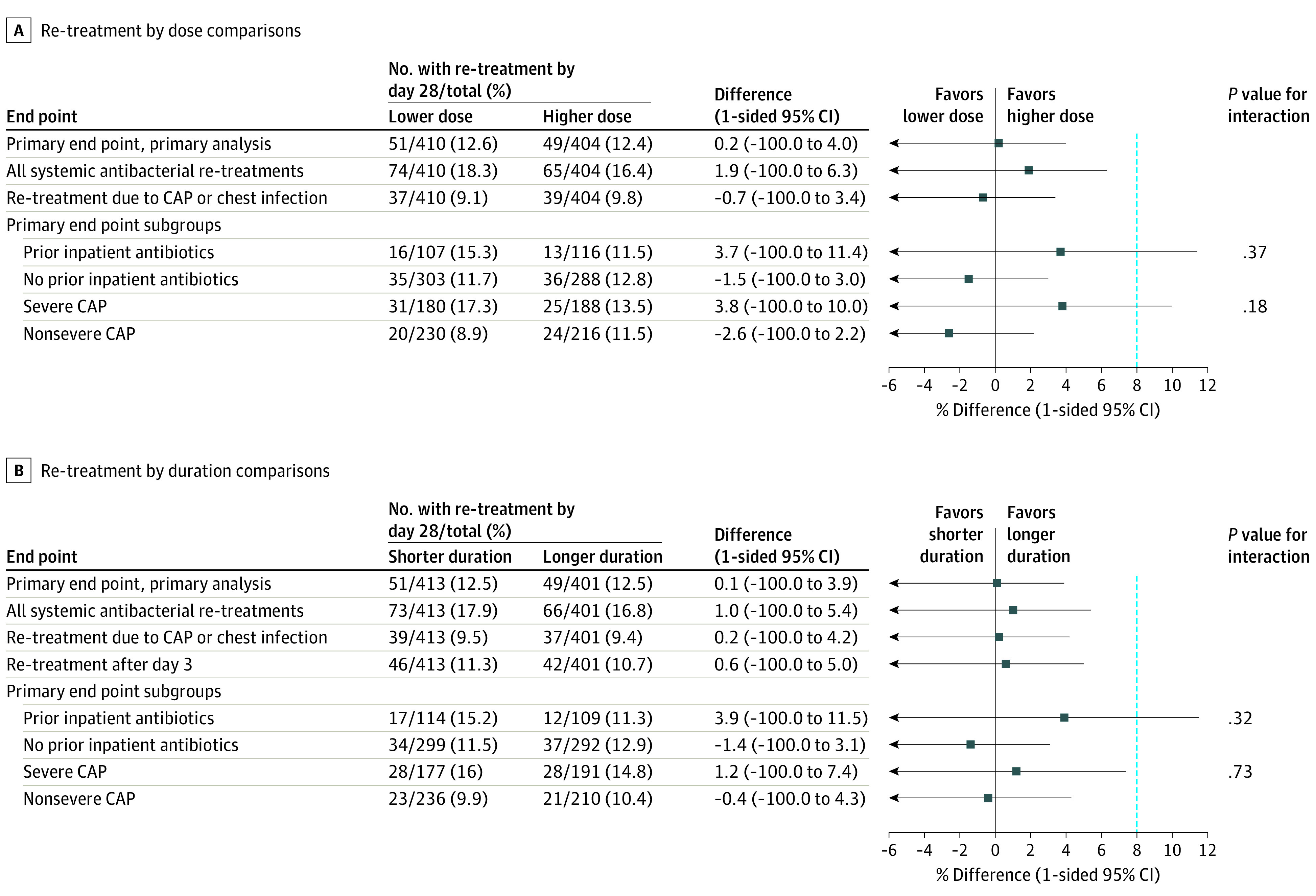
Main outcomes and measures: The primary outcome was clinically indicated antibiotic re-treatment for respiratory infection within 28 days after randomization. The noninferiority margin was 8%. Secondary outcomes included severity/duration of 9 parent-reported CAP symptoms, 3 antibiotic-related adverse events, and phenotypic resistance in colonizing Streptococcus pneumoniae isolates.
Results: Of 824 participants randomized into 1 of the 4 groups, 814 received at least 1 dose of trial medication (median [IQR] age, 2.5 years [1.6-2.7]; 421 [52%] males and 393 [48%] females), and the primary outcome was available for 789 (97%). For lower vs higher dose, the primary outcome occurred in 12.6% with lower dose vs 12.4% with higher dose (difference, 0.2% [1-sided 95% CI -∞ to 4.0%]), and in 12.5% with 3-day treatment vs 12.5% with 7-day treatment (difference, 0.1% [1-sided 95% CI -∞ to 3.9]). Both groups demonstrated noninferiority with no significant interaction between dose and duration (P = .63). Of the 14 prespecified secondary end points, the only significant differences were 3-day vs 7-day treatment for cough duration (median 12 days vs 10 days; hazard ratio [HR], 1.2 [95% CI, 1.0 to 1.4]; P = .04) and sleep disturbed by cough (median, 4 days vs 4 days; HR, 1.2 [95% CI, 1.0 to 1.4]; P = .03). Among the subgroup of children with severe CAP, the primary end point occurred in 17.3% of lower-dose recipients vs 13.5% of higher-dose recipients (difference, 3.8% [1-sided 95% CI, -∞ to10%]; P value for interaction = .18) and in 16.0% with 3-day treatment vs 14.8% with 7-day treatment (difference, 1.2% [1-sided 95% CI, -∞ to 7.4%]; P value for interaction = .73).
Conclusions and relevance: Among children with CAP discharged from an emergency department or hospital ward (within 48 hours), lower-dose outpatient oral amoxicillin was noninferior to higher dose, and 3-day duration was noninferior to 7 days, with regard to need for antibiotic re-treatment. However, disease severity, treatment setting, prior antibiotics received, and acceptability of the noninferiority margin require consideration when interpreting the findings.
Trial registration: ISRCTN Identifier: ISRCTN76888927.
Conflict of interest statement
Figures
Comment in
-
Amoxicillin Dose and Duration of Treatment and Need for Antibiotic Re-treatment in Children With Community-Acquired Pneumonia.JAMA. 2022 Mar 15;327(11):1089-1090. doi: 10.1001/jama.2022.1022. JAMA. 2022. PMID: 35289887 No abstract available.
-
Antibiotics for Pediatric Pneumonia: Might Less Be Enough?: June 2022 Annals of Emergency Medicine Journal Club.Ann Emerg Med. 2022 Jun;79(6):573-575. doi: 10.1016/j.annemergmed.2022.04.001. Ann Emerg Med. 2022. PMID: 35569895 No abstract available.
References
-
- van de Maat J, van de Voort E, Mintegi S, et al. ; Research in European Pediatric Emergency Medicine study group . Antibiotic prescription for febrile children in European emergency departments: a cross-sectional, observational study. Lancet Infect Dis. 2019;19(4):382-391. doi:10.1016/S1473-3099(18)30672-8 - DOI - PubMed
-
- Verbakel JY, Van den Bruel A, Thompson M, et al. ; European Research Network on Recognising Serious Infection (ERNIE) . How well do clinical prediction rules perform in identifying serious infections in acutely ill children across an international network of ambulatory care datasets? BMC Med. 2013;11(1):10. doi:10.1186/1741-7015-11-10 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
